

Pirfenidone Reduces Respiratory-related Hospitalizations in Idiopathic Pulmonary Fibrosis
- PMID: 28471697
- PMCID: PMC5620679
- DOI: 10.1164/rccm.201701-0091OC
Pirfenidone Reduces Respiratory-related Hospitalizations in Idiopathic Pulmonary Fibrosis
Abstract
Rationale: Respiratory-related hospitalizations of patients with idiopathic pulmonary fibrosis (IPF) are more frequent than those for acute IPF exacerbations and are associated with poor outcomes.
Objectives: To compare the risk of nonelective hospitalization by type (all-cause, respiratory related, and non-respiratory related) and death after hospitalization with use of pirfenidone versus placebo over 52 weeks using data derived from three phase III IPF clinical trials.
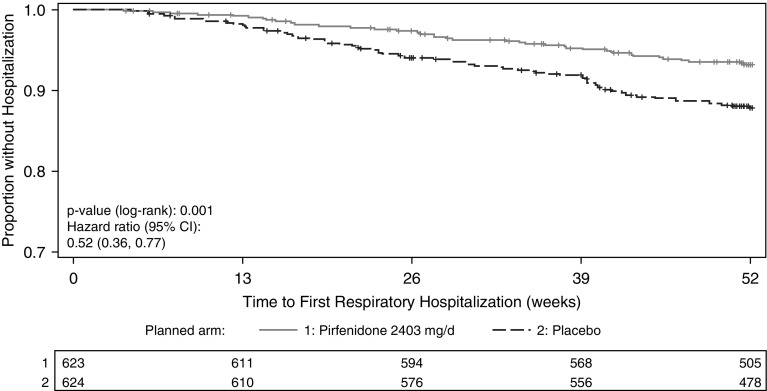
Methods: Individual patient data was pooled from three phase III randomized, placebo-controlled studies of pirfenidone for IPF (the two CAPACITY [Clinical Studies Assessing Pirfenidone in IPF: Research of Efficacy and Safety Outcomes] trials and the ASCEND [Assessment of Pirfenidone to Confirm Efficacy and Safety in Idiopathic Pulmonary Fibrosis] trial), including all patients randomized to pirfenidone 2,403 mg/d (n = 623) or placebo (n = 624). The risk of hospitalization over 52 weeks was compared using standard time-to-event methods. Among those hospitalized, the risk of death after hospitalization was compared with adjustment for treatment group propensity.
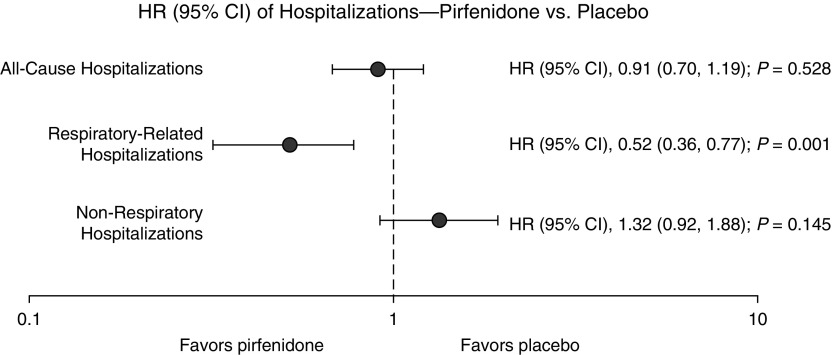
Measurements and main results: A total of 1,247 patients (692 from the CAPACITY trials and 555 from the ASCEND trial) were included in the pooled analysis. Pirfenidone was associated with lower risk of respiratory-related hospitalization than placebo (7% vs. 12%; hazard ratio [HR], 0.52; 95% confidence interval [CI], 0.36-0.77; P = 0.001), but all-cause (HR, 0.91; 95% CI, 0.70-1.19; P = 0.528) or non-respiratory-related hospitalization (HR, 1.32; 95% CI, 0.92-1.88; P = 0.145) was not. Among those hospitalized for any reason, treatment with pirfenidone was associated with lower risk of death after hospitalization up to 52 weeks after randomization, but this association was no longer significant with longer follow-up.
Conclusions: In a pooled analysis of three phase III IPF clinical trials, patients receiving pirfenidone had a lower risk of nonelective respiratory-related hospitalization over the course of 1 year. The effect of pirfenidone on death after hospitalization is uncertain.
Keywords: hospitalization; idiopathic pulmonary fibrosis; mortality; pirfenidone.
Figures
Comment in
-
Patient-centered Outcomes in Idiopathic Pulmonary Fibrosis Clinical Trials.Am J Respir Crit Care Med. 2017 Sep 15;196(6):674-675. doi: 10.1164/rccm.201705-0975ED. Am J Respir Crit Care Med. 2017. PMID: 28609111 Free PMC article. No abstract available.
References
-
- Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, Colby TV, Cordier JF, Flaherty KR, Lasky JA, et al. ATS/ERS/JRS/ALAT Committee on Idiopathic Pulmonary Fibrosis. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183:788–824. - PMC - PubMed
-
- Collard HR, Ward AJ, Lanes S, Cortney Hayflinger D, Rosenberg DM, Hunsche E. Burden of illness in idiopathic pulmonary fibrosis. J Med Econ. 2012;15:829–835. - PubMed
-
- Collard HR, Chen SY, Yeh WS, Li Q, Lee YC, Wang A, Raghu G. Health care utilization and costs of idiopathic pulmonary fibrosis in U.S. Medicare beneficiaries aged 65 years and older. Ann Am Thorac Soc. 2015;12:981–987. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
