

Comparisons of Noninvasive Methods Used to Assess Exercise Stroke Volume in Heart Failure with Preserved Ejection Fraction
- PMID: 28471812
- PMCID: PMC5561476
- DOI: 10.1249/MSS.0000000000001308
Comparisons of Noninvasive Methods Used to Assess Exercise Stroke Volume in Heart Failure with Preserved Ejection Fraction
Abstract
Introduction: Cardiopulmonary exercise testing (CPET) plays an important role in properly phenotyping signs and symptoms of heart failure with preserved ejection fraction (HFpEF). The prognostic value of CPET is strengthened when accompanied by cardiac hemodynamic measurements. Although recognized as the "gold" standard, cardiac catheterization is impractical for routine CPET. Thus, advancing the scientific/methodologic understanding of noninvasive techniques for exercise cardiac hemodynamic assessment is clinically impactful in HFpEF. This study tested the concurrent validity of noninvasive acetylene gas (C2H2) uptake, echocardiography (ECHO), and oxygen pulse (O2pulse) for measuring/predicting exercise stroke volume (SV) in HFpEF.
Methods: Eighteen white HFpEF and 18 age-/sex-matched healthy controls participated in upright CPET (ages, 69 ± 9 yr vs 63 ± 9 yr). At rest, 20 W, and peak exercise, SV was measured at steady-state via C2H2 rebreathe (SVACET) and ECHO (SVECHO), whereas O2pulse was derived (=V˙O2/HR).
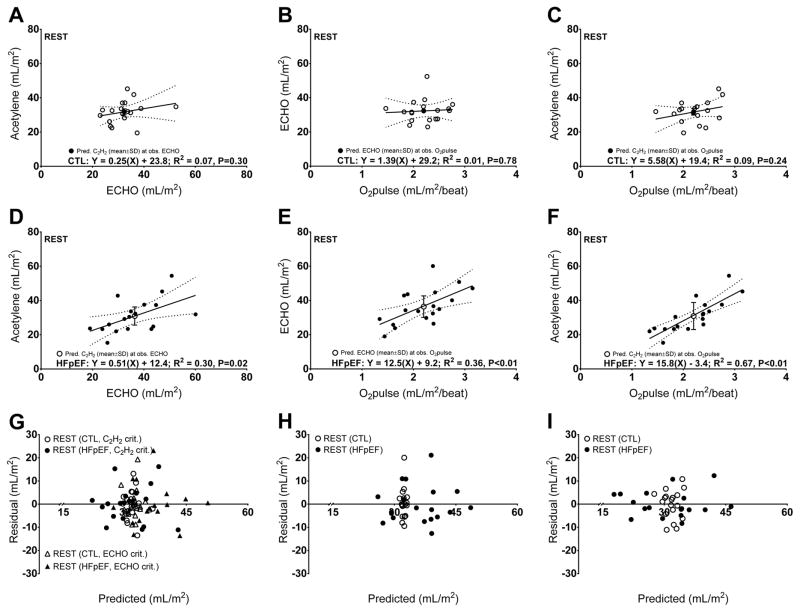
Results: Resting relationships between SVACET and SVECHO, SVECHO and O2pulse, or SVACET and O2pulse were significant in HFpEF (R = 0.30, 0.36, 0.67), but not controls (R = 0.07, 0.01, 0.09), respectively. Resting relationships persisted to 20 W in HFpEF (R = 0.70, 0.53, 0.70) and controls (R = 0.05, 0.07, 0.21), respectively. Peak exercise relationships were significant in HFpEF (R = 0.62, 0.24, 0.64), but only for SVACET versus O2pulse in controls (R = 0.07, 0.04, 0.33), respectively. Standardized standard error of estimate between techniques was strongest in HFpEF at 20 W: SVACET versus SVECHO = 0.57 ± 0.22; SVECHO versus O2pulse = 0.71 ± 0.28; SVACET versus O2pulse = 0.56 ± 0.22.
Conclusions: Constituting a clinically impactful step towards construct validation testing, these data suggest SVACET, SVECHO, and O2pulse demonstrate moderate-to-strong concurrent validity for measuring/predicting exercise SV in HFpEF.
Conflict of interest statement
The authors declare no conflicts of interest. The results of the present study do not constitute endorsement by ACSM. The results of the study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation.
Figures


Similar articles
-
Exercise Stroke Volume in Adult Cystic Fibrosis: A Comparison of Acetylene Pulmonary Uptake and Oxygen Pulse.Clin Med Insights Circ Respir Pulm Med. 2018 Jul 25;12:1179548418790564. doi: 10.1177/1179548418790564. eCollection 2018. Clin Med Insights Circ Respir Pulm Med. 2018. PMID: 30083061 Free PMC article.
-
The combined exercise stress echocardiography and cardiopulmonary exercise test for identification of masked heart failure with preserved ejection fraction in patients with hypertension.Eur J Prev Cardiol. 2016 Jan;23(1):71-7. doi: 10.1177/2047487315604836. Epub 2015 Sep 10. Eur J Prev Cardiol. 2016. PMID: 26358991
-
Impaired myocardial oxygen availability contributes to abnormal exercise hemodynamics in heart failure with preserved ejection fraction.J Am Heart Assoc. 2014 Dec 2;3(6):e001293. doi: 10.1161/JAHA.114.001293. J Am Heart Assoc. 2014. PMID: 25468660 Free PMC article.
-
(Non)-Exertional Variables of Cardiopulmonary Exercise Testing in Heart Failure with and Without Cardiac Amyloidosis.Curr Heart Fail Rep. 2024 Jun;21(3):224-237. doi: 10.1007/s11897-024-00661-1. Epub 2024 Apr 18. Curr Heart Fail Rep. 2024. PMID: 38635117 Free PMC article. Review.
-
Cardiopulmonary Exercise Testing: What Is its Value?J Am Coll Cardiol. 2017 Sep 26;70(13):1618-1636. doi: 10.1016/j.jacc.2017.08.012. J Am Coll Cardiol. 2017. PMID: 28935040 Review.
Cited by
-
A Novel Three-Dimensional and Tissue Doppler Echocardiographic Index for Diagnosing and Prognosticating Heart Failure With Preserved Ejection Fraction.Front Cardiovasc Med. 2022 Feb 10;9:822314. doi: 10.3389/fcvm.2022.822314. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35224053 Free PMC article.
-
Alveolar Air and O2 Uptake During Exercise in Patients With Heart Failure.J Card Fail. 2018 Oct;24(10):695-705. doi: 10.1016/j.cardfail.2018.08.001. Epub 2018 Aug 10. J Card Fail. 2018. PMID: 30103021 Free PMC article.
-
Impaired central hemodynamics in chronic obstructive pulmonary disease during submaximal exercise.J Appl Physiol (1985). 2019 Sep 1;127(3):691-697. doi: 10.1152/japplphysiol.00877.2018. Epub 2019 Jul 11. J Appl Physiol (1985). 2019. PMID: 31295068 Free PMC article.
-
Echocardiographic Detection of Occult Diastolic Dysfunction in Pulmonary Hypertension After Fluid Challenge.J Am Heart Assoc. 2019 Sep 3;8(17):e012504. doi: 10.1161/JAHA.119.012504. Epub 2019 Aug 31. J Am Heart Assoc. 2019. PMID: 31475602 Free PMC article.
-
Exercise Stroke Volume in Adult Cystic Fibrosis: A Comparison of Acetylene Pulmonary Uptake and Oxygen Pulse.Clin Med Insights Circ Respir Pulm Med. 2018 Jul 25;12:1179548418790564. doi: 10.1177/1179548418790564. eCollection 2018. Clin Med Insights Circ Respir Pulm Med. 2018. PMID: 30083061 Free PMC article.
References
-
- Agostoni P, Cattadori G, Apostolo A, et al. Noninvasive measurement of cardiac output during exercise by inert gas rebreathing technique: a new tool for heart failure evaluation. J Am Coll Cardiol. 2005;46(9):1779–81. - PubMed
-
- Babu SC, Piccorelli GO, Shah PM, Stein JH, Clauss RH. Incidence and Results of Arterial Complications among 16,350 Patients Undergoing Cardiac-Catheterization. Journal of Vascular Surgery. 1989;10(2):113–6. - PubMed
-
- Bhambhani Y, Norris S, Bell G. Prediction of stroke volume from oxygen pulse measurements in untrained and trained men. Can J Appl Physiol. 1994;19(1):49–59. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
