

Comparative analysis of diagnostic performance, feasibility and cost of different test-methods for thyroid nodules with indeterminate cytology
- PMID: 28472764
- PMCID: PMC5564779
- DOI: 10.18632/oncotarget.17220
Comparative analysis of diagnostic performance, feasibility and cost of different test-methods for thyroid nodules with indeterminate cytology
Abstract
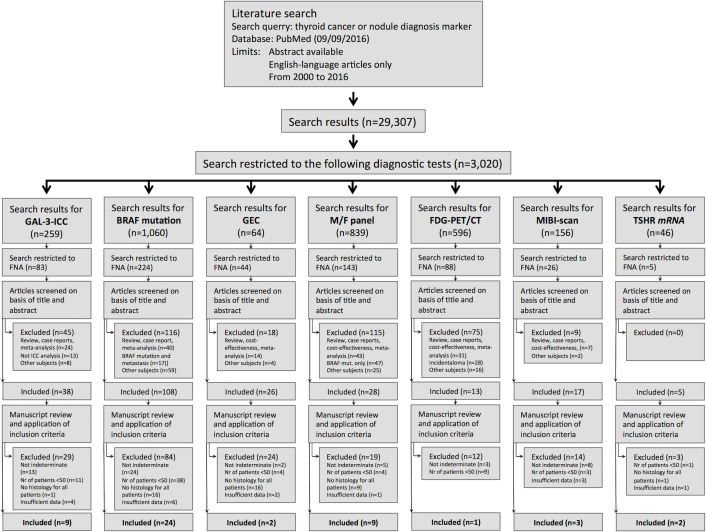
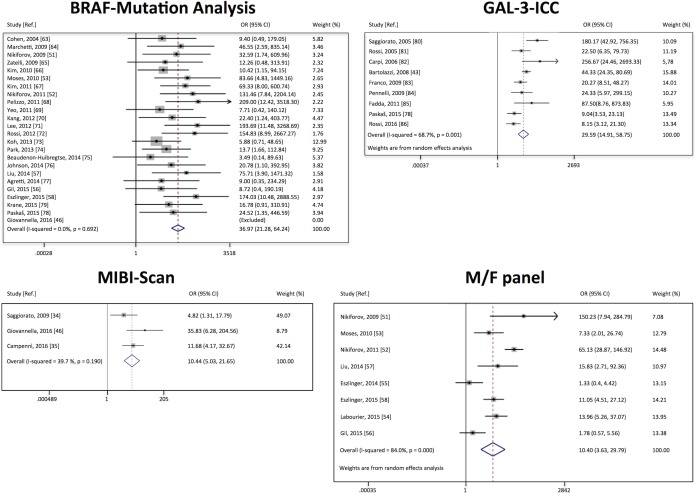
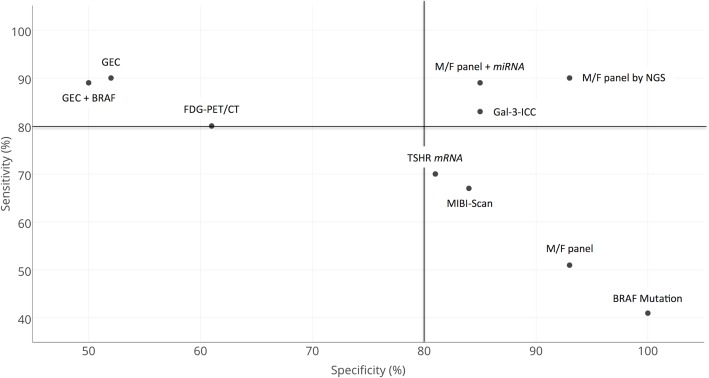
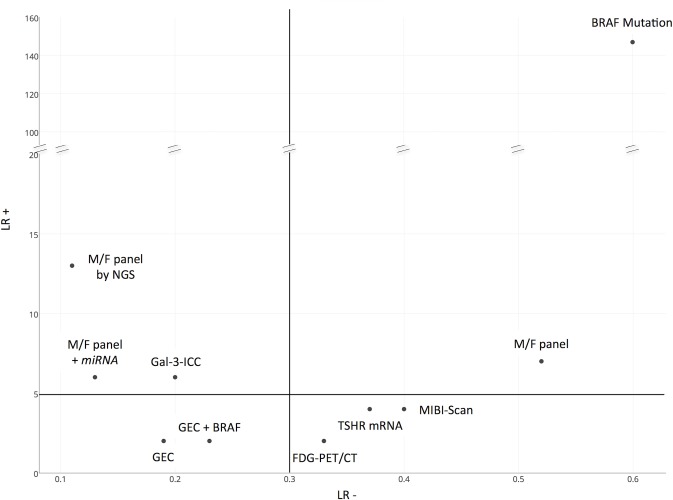
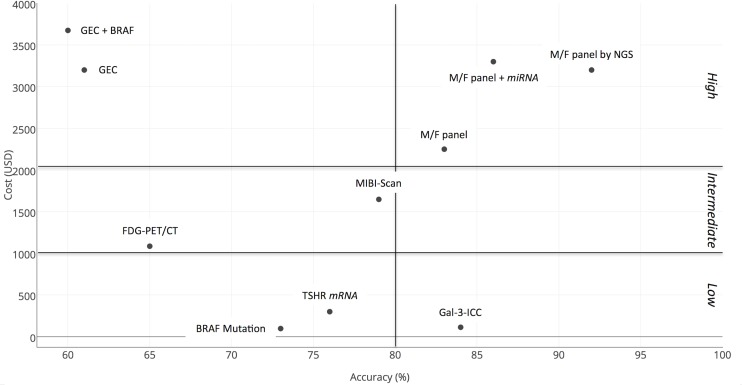
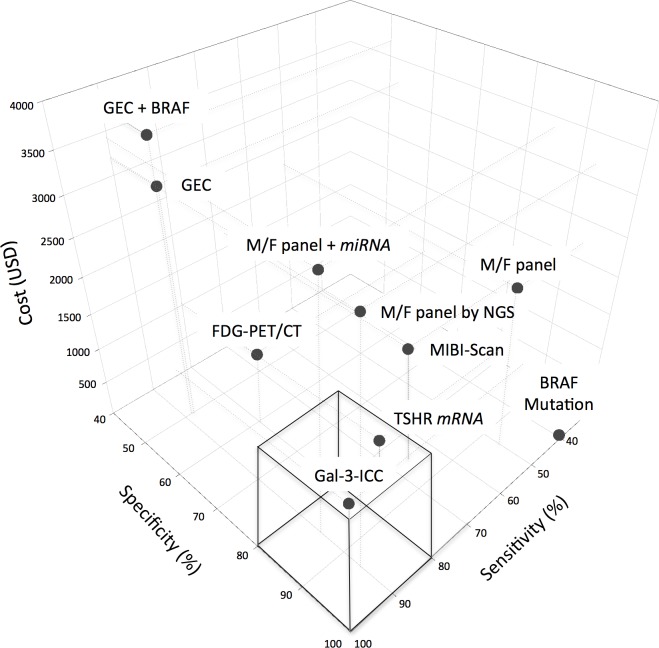
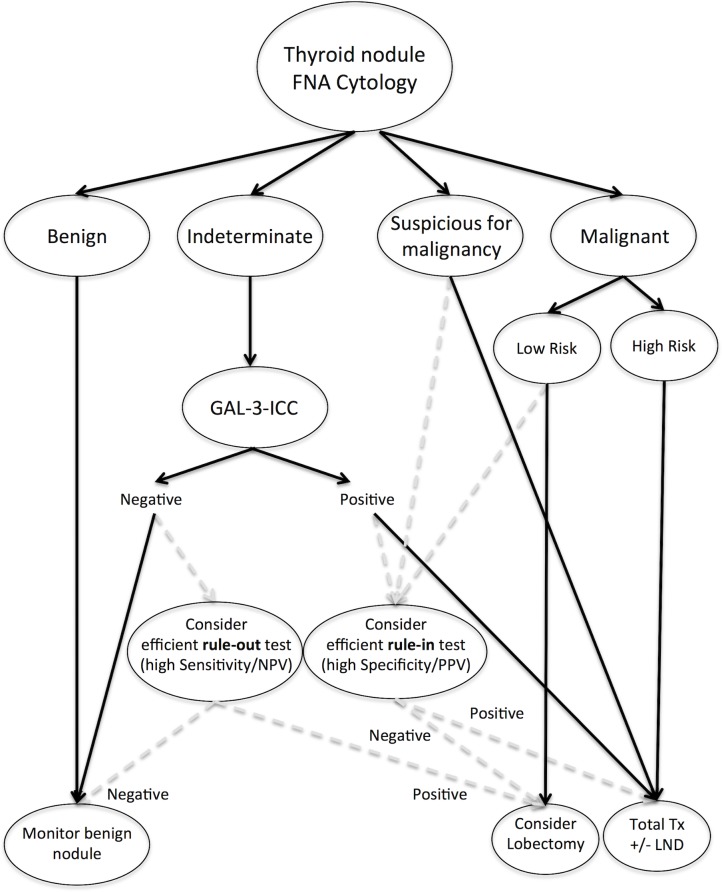
Since it is impossible to recognize malignancy at fine needle aspiration (FNA) cytology in indeterminate thyroid nodules, surgery is recommended for all of them. However, cancer rate at final histology is <30%. Many different test-methods have been proposed to increase diagnostic accuracy in such lesions, including Galectin-3-ICC (GAL-3-ICC), BRAF mutation analysis (BRAF), Gene Expression Classifier (GEC) alone and GEC+BRAF, mutation/fusion (M/F) panel, alone, M/F panel+miRNA GEC, and M/F panel by next generation sequencing (NGS), FDG-PET/CT, MIBI-Scan and TSHR mRNA blood assay.We performed systematic reviews and meta-analyses to compare their features, feasibility, diagnostic performance and cost. GEC, GEC+BRAF, M/F panel+miRNA GEC and M/F panel by NGS were the best in ruling-out malignancy (sensitivity = 90%, 89%, 89% and 90% respectively). BRAF and M/F panel alone and by NGS were the best in ruling-in malignancy (specificity = 100%, 93% and 93%). The M/F by NGS showed the highest accuracy (92%) and BRAF the highest diagnostic odds ratio (DOR) (247). GAL-3-ICC performed well as rule-out (sensitivity = 83%) and rule-in test (specificity = 85%), with good accuracy (84%) and high DOR (27) and is one of the cheapest (113 USD) and easiest one to be performed in different clinical settings.In conclusion, the more accurate molecular-based test-methods are still expensive and restricted to few, highly specialized and centralized laboratories. GAL-3-ICC, although limited by some false negatives, represents the most suitable screening test-method to be applied on a large-scale basis in the diagnostic algorithm of indeterminate thyroid lesions.
Keywords: diagnostic performance; indeterminate thyroid nodules; meta-analysis; systematic review; thyroid FNA cytology.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Perros P, Boelaert K, Colley S, Evans C, Evans RM, Gerrard Ba G, Gilbert J, Harrison B, Johnson SJ, Giles TE, Moss L, Lewington V, Newbold K, et al. Guidelines for the management of thyroid cancer. Clin Endocrinol (Oxf) 2014;81:1–122. - PubMed
-
- Cibas ES, Ali SZ. The Bethesda System for Reporting Thyroid Cytopathology. Thyroid. 2009;19:1159–65. - PubMed
-
- Nardi F, Basolo F, Crescenzi A, Fadda G, Frasoldati A, Orlandi F, Palombini L, Papini E, Zini M, Pontecorvi A, Vitti P. Italian consensus for the classification and reporting of thyroid cytology. J Endocrinol Invest. 2014;37:593–99. - PubMed
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1–133. - PMC - PubMed
-
- Baloch ZW, Fleisher S, LiVolsi VA, Gupta PK. Diagnosis of “follicular neoplasm”: a gray zone in thyroid fine-needle aspiration cytology. Diagn Cytopathol. 2002;26:41–44. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
