

Humanized monoclonal antibody armanezumab specific to N-terminus of pathological tau: characterization and therapeutic potency
- PMID: 28472993
- PMCID: PMC5418694
- DOI: 10.1186/s13024-017-0172-1
Humanized monoclonal antibody armanezumab specific to N-terminus of pathological tau: characterization and therapeutic potency
Abstract
Background: The experience from clinical trials indicates that anti-Aβ immunotherapy could be effective in early/pre-clinical stages of AD, whereas at the late stages promoting the clearing of Aβ alone may be insufficient to halt the disease progression. At the same time, pathological tau correlates much better with the degree of dementia than Aβ deposition. Therefore, targeting pathological tau may provide a more promising approach for the treatment of advanced stages of AD. Recent data demonstrates that the N-terminal region of tau spanning aa 2-18 termed "phosphatase activation domain" that is normally hidden in the native protein in 'paperclip'-like conformation, becomes exposed in pathological tau and plays an essential role in the inhibition of fast axonal transport and in aggregation of tau. Hence, we hypothesized that anti-Tau2-18 monoclonal antibodies (mAb) may recognize pathological, but not normal tau at very early stages of tauopathy and prevent or decrease the aggregation of this molecule.
Methods: Mouse mAbs were generated using standard hybridoma methodology. CDR grafting was used for humanization of mouse mAb. Humanized mAb (Armanezumab) was characterized and tested in vitro/ex vivo/in vivo using biochemical and immunological methods (HPLC, Biacore, ELISA, IHC, FRET, etc.). Stable DG44 cell line expressing Armanezumab was generated by clone selection with increased concentrations of methotrexate (MTX).
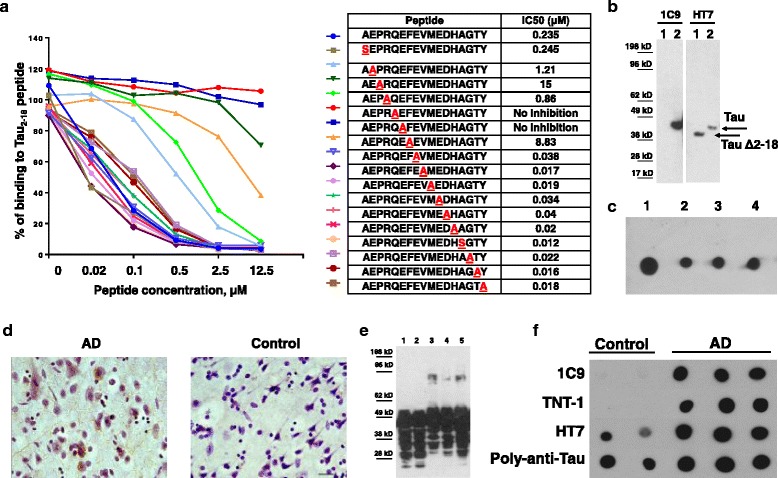
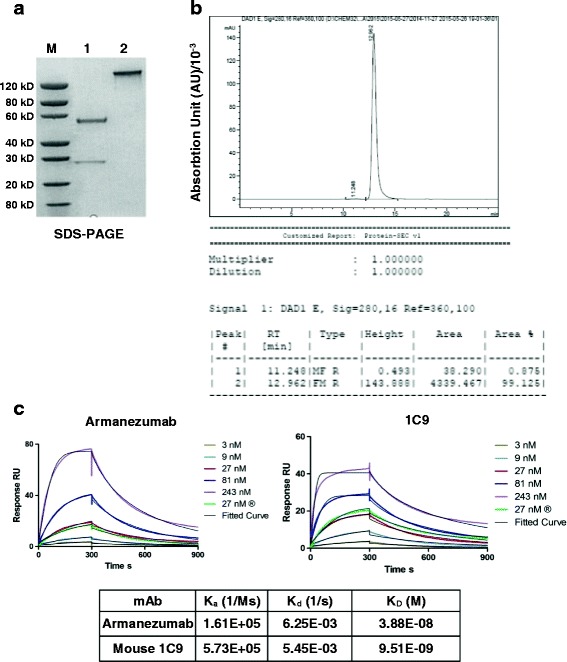
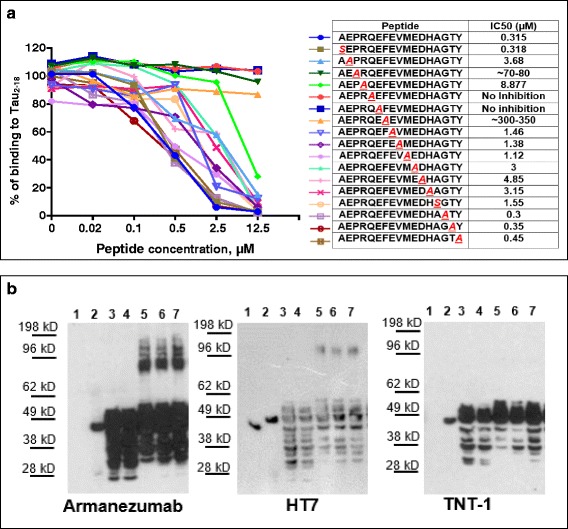
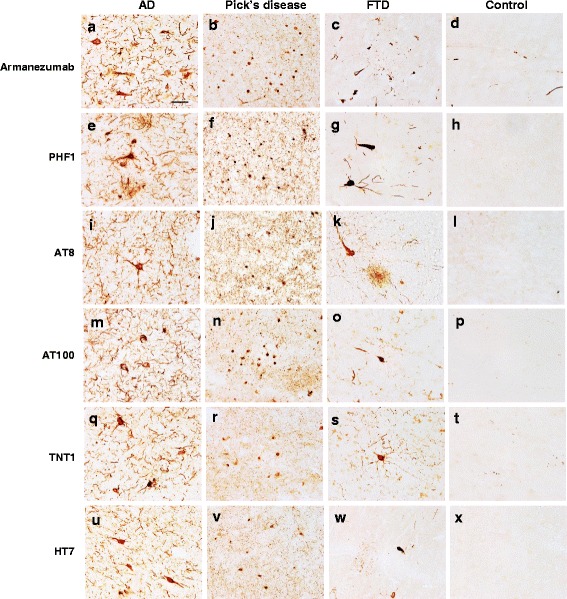
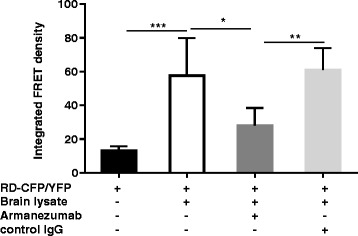
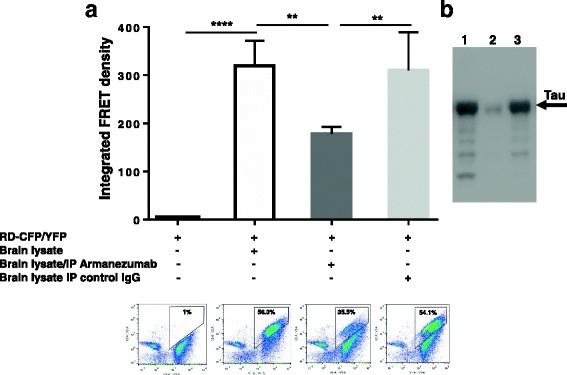
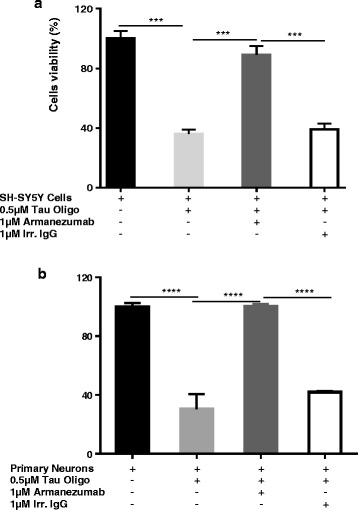
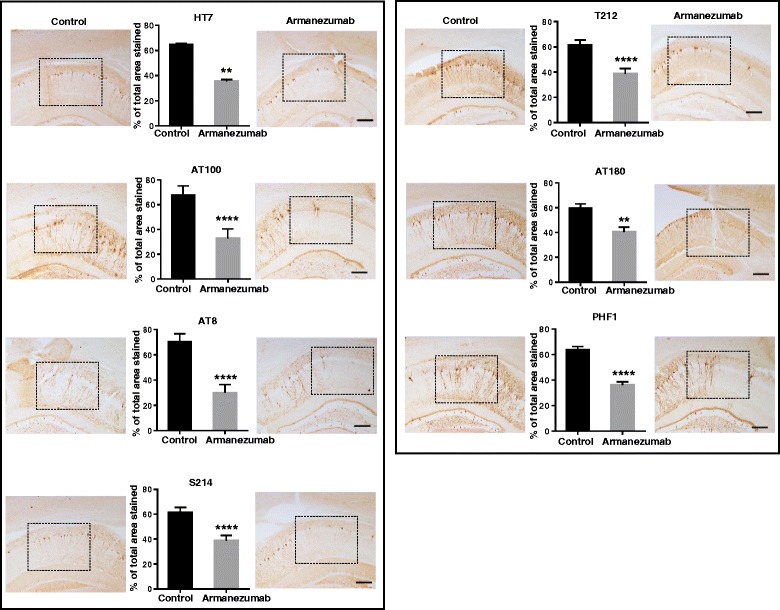
Results: A panel of mouse mAbs was generated, clone 1C9 was selected based on binding to pathological human tau with high affinity and humanized. Fine epitope mapping revealed conservation of the epitope of human tau recognized by the parent murine mAb and Armanezumab. Importantly, Armanezumab (i) bound to tau with high affinity as determined by Biacore; (ii) bound pathological tau in brains from AD, FTD and Pick's disease cases; (iii) inhibited seeding effect of aggregated tau from brain lysate of P301S Tg mice; (iv) inhibited cytotoxic effect of tau oligomers; (v) reduced total tau (HT7) and AT100, PHF1, AT8, AT180, p212, p214-positive tau species in brains of tau transgenic mice after intracranial injection. A stable CHO cell line producing >1.5 g/l humanized mAb, Armanezumab was generated.
Conclusion: These findings suggest that Armanezumab could be therapeutic in clinical studies for treatment of AD.
Keywords: Alzheimer’s disease; Humanization; Immunotherapy; Monoclonal antibody; Phosphatase activation domain; Tauopathy; Therapeutic efficacy.
Figures
References
-
- Schneider LS, Mangialasche F, Andreasen N, Feldman H, Giacobini E, Jones R, Mantua V, Mecocci P, Pani L, Winblad B, Kivipelto M. Clinical trials and late-stage drug development for Alzheimer’s disease: an appraisal from 1984 to 2014. J Intern Med. 2014;275:251–283. doi: 10.1111/joim.12191. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
