

Underuse of Prevention and Lifestyle Counseling in Patients With Peripheral Artery Disease
- PMID: 28473134
- PMCID: PMC5497594
- DOI: 10.1016/j.jacc.2017.02.064
Underuse of Prevention and Lifestyle Counseling in Patients With Peripheral Artery Disease
Abstract
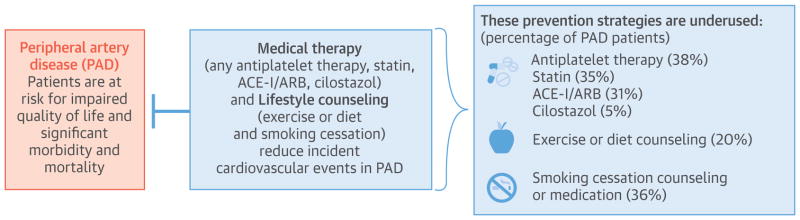
Background: Little is known about patterns of medication use and lifestyle counseling in patients with peripheral artery disease (PAD) in the United States.
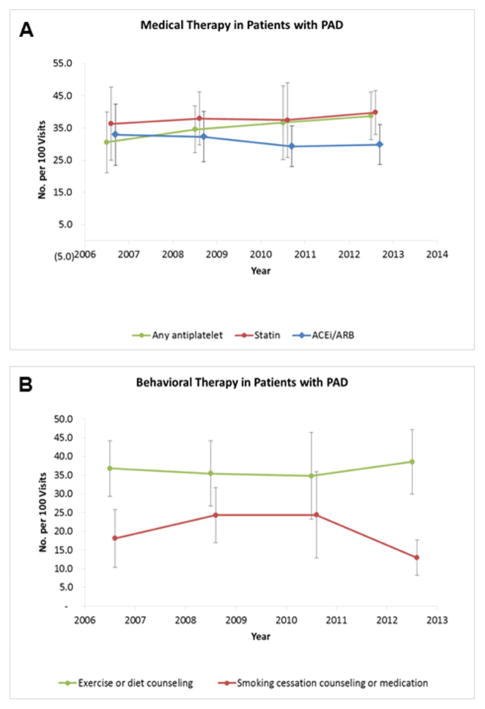
Objectives: The authors sought to evaluate trends in both medical therapy and lifestyle counseling for PAD patients in the United States from 2005 through 2012.
Methods: Data from 1,982 outpatient visits among patients with PAD were obtained from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey, a nationally representative assessment of office-based and hospital outpatient department practice. Trends in the proportion of visits with medication use (antiplatelet therapy, statins, angiotensin-converting enzyme inhibitors [ACEIs] or angiotensin receptor blockers [ARBs], and cilostazol) and lifestyle counseling (exercise or diet counseling and smoking cessation) were evaluated.
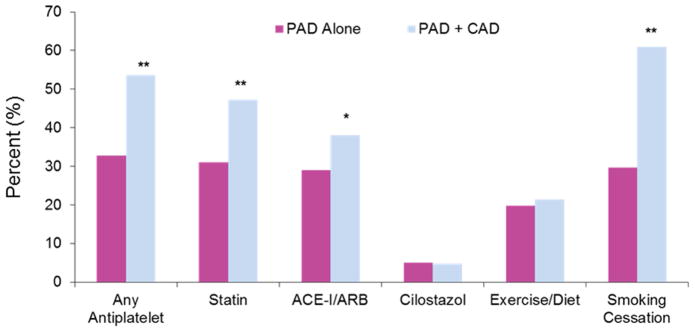
Results: Over the 8-year period, the average annual number of ambulatory visits in the United States for PAD was 3,883,665. Across all visits, mean age was 69.2 years, 51.8% were female, and 56.6% were non-Hispanic white. Comorbid coronary artery disease (CAD) was present in 24.3% of visits. Medication use for cardiovascular prevention and symptoms of claudication was low: any antiplatelet therapy in 35.7% (standard error [SE]: 2.7%), statin in 33.1% (SE: 2.4%), ACEI/ARB in 28.4% (SE: 2.0%), and cilostazol in 4.7% (SE: 1.0%) of visits. Exercise or diet counseling was used in 22% (SE: 2.3%) of visits. Among current smokers with PAD, smoking cessation counseling or medication was used in 35.8% (SE: 4.6%) of visits. There was no significant change in medication use or lifestyle counseling over time. Compared with visits for patients with PAD alone, comorbid PAD and CAD were more likely to be prescribed antiplatelet therapy (odds ratio [OR]: 2.6; 95% confidence interval [CI]: 1.8 to 3.9), statins (OR: 2.6; 95% CI: 1.8 to 3.9), ACEI/ARB (OR: 2.6; 95% CI: 1.8 to 3.9), and smoking cessation counseling (OR: 4.4; 95% CI: 2.0 to 9.6).
Conclusions: The use of guideline-recommended therapies in patients with PAD was much lower than expected, which highlights an opportunity to improve the quality of care in these high-risk patients.
Keywords: PAD; cardiovascular prevention; epidemiology; lifestyle.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Treatment Gap in Peripheral Artery Disease.J Am Coll Cardiol. 2017 May 9;69(18):2301-2303. doi: 10.1016/j.jacc.2017.03.024. J Am Coll Cardiol. 2017. PMID: 28473135 No abstract available.
References
-
- Fowkes FG, Rudan D, Rudan I, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382:1329–40. - PubMed
-
- Savji N, Rockman CB, Skolnick AH, et al. Association between advanced age and vascular disease in different arterial territories: a population database of over 3. 6 million subjects. J Am Coll Cardiol. 2013;61:1736–43. - PubMed
-
- Writing Group M. Mozaffarian D, Benjamin EJ, et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016;133:e38–360. - PubMed
-
- Criqui MH, Aboyans V. Epidemiology of peripheral artery disease. Circ Res. 2015;116:1509–26. - PubMed
-
- Subherwal S, Patel MR, Kober L, et al. Peripheral artery disease is a coronary heart disease risk equivalent among both men and women: results from a nationwide study. Eur J Prev Cardiol. 2015;22:317–25. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
