

Combined Anti-VEGF and Anti-CTLA-4 Therapy Elicits Humoral Immunity to Galectin-1 Which Is Associated with Favorable Clinical Outcomes
- PMID: 28473314
- PMCID: PMC5509159
- DOI: 10.1158/2326-6066.CIR-16-0385
Combined Anti-VEGF and Anti-CTLA-4 Therapy Elicits Humoral Immunity to Galectin-1 Which Is Associated with Favorable Clinical Outcomes
Abstract
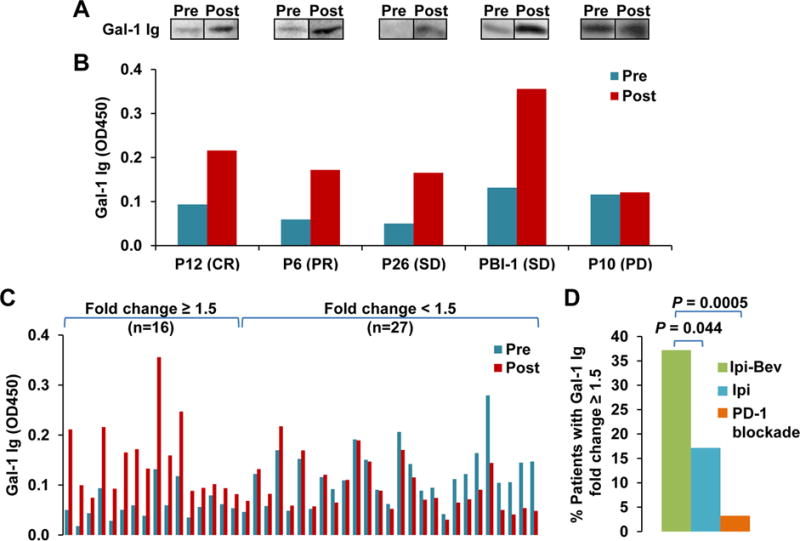
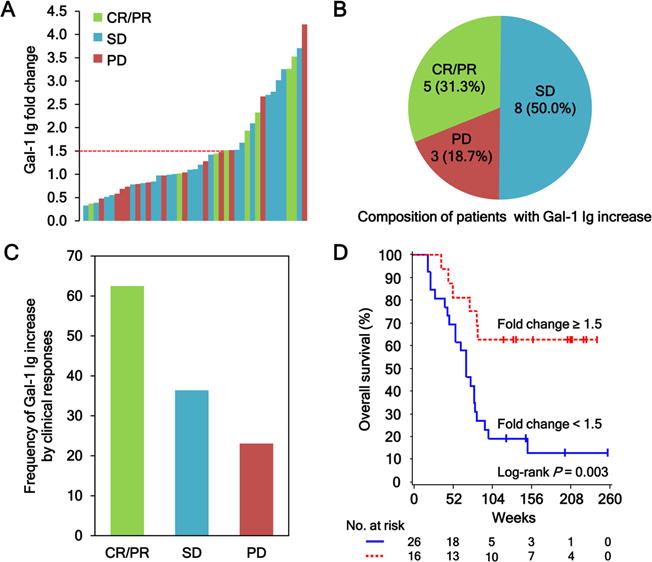
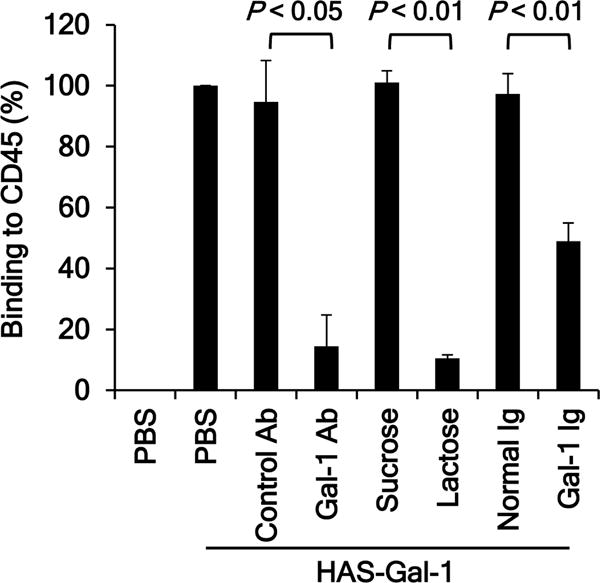
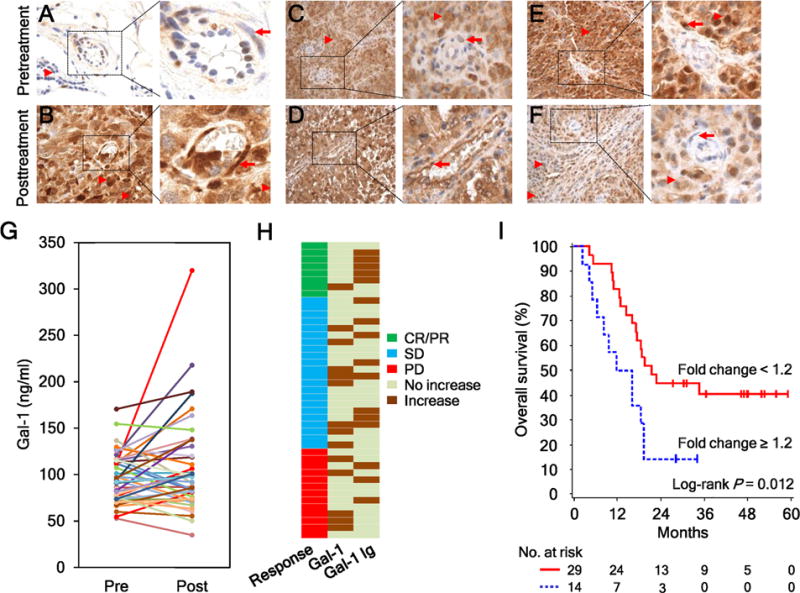
The combination of anti-VEGF blockade (bevacizumab) with immune checkpoint anti-CTLA-4 blockade (ipilimumab) in a phase I study showed tumor endothelial activation and immune cell infiltration that were associated with favorable clinical outcomes in patients with metastatic melanoma. To identify potential immune targets responsible for these observations, posttreatment plasma from long-term responding patients were used to screen human protein arrays. We reported that ipilimumab plus bevacizumab therapy elicited humoral immune responses to galectin-1 (Gal-1), which exhibits protumor, proangiogenesis, and immunosuppressive activities in 37.2% of treated patients. Gal-1 antibodies purified from posttreatment plasma suppressed the binding of Gal-1 to CD45, a T-cell surface receptor that transduces apoptotic signals upon binding to extracellular Gal-1. Antibody responses to Gal-1 were found more frequently in the group of patients with therapeutic responses and correlated with improved overall survival. In contrast, another subgroup of treated patients had increased circulating Gal-1 protein instead, and they had reduced overall survival. Our findings suggest that humoral immunity to Gal-1 may contribute to the efficacy of anti-VEGF and anti-CTLA-4 combination therapy. Gal-1 may offer an additional therapeutic target linking anti-angiogenesis and immune checkpoint blockade. Cancer Immunol Res; 5(6); 446-54. ©2017 AACR.
©2017 American Association for Cancer Research.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
