

Initiation Patterns of Statins in the 2 Years After Release of the 2013 American College of Cardiology/American Heart Association (ACC/AHA) Cholesterol Management Guideline in a Large US Health Plan
- PMID: 28473405
- PMCID: PMC5524081
- DOI: 10.1161/JAHA.116.005205
Initiation Patterns of Statins in the 2 Years After Release of the 2013 American College of Cardiology/American Heart Association (ACC/AHA) Cholesterol Management Guideline in a Large US Health Plan
Abstract
Background: The purpose of this study was to characterize changes in statin utilization patterns in patients newly initiated on therapy in the 2 years following the release of the 2013 American College of Cardiology/American Heart Association (ACC/AHA) cholesterol management guideline in a large US health plan population.
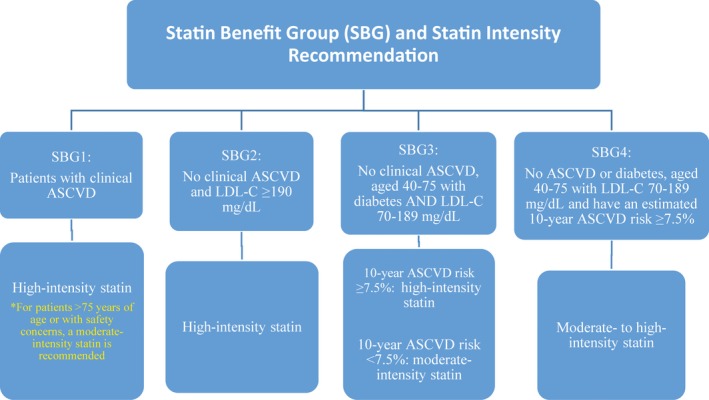
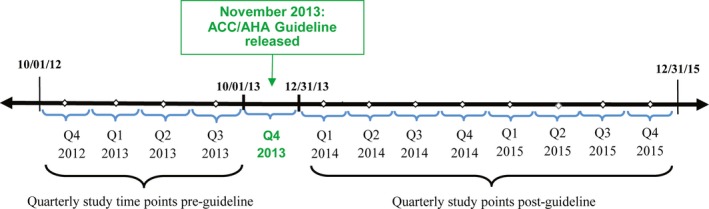
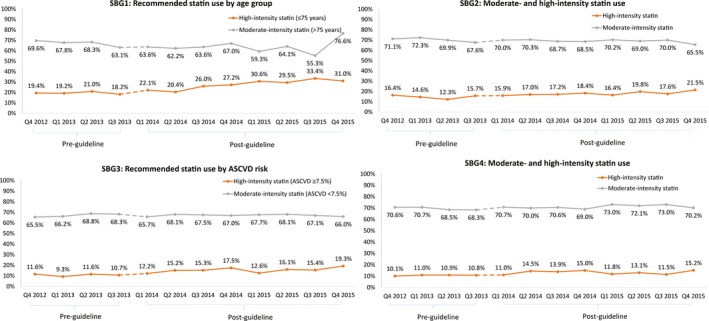
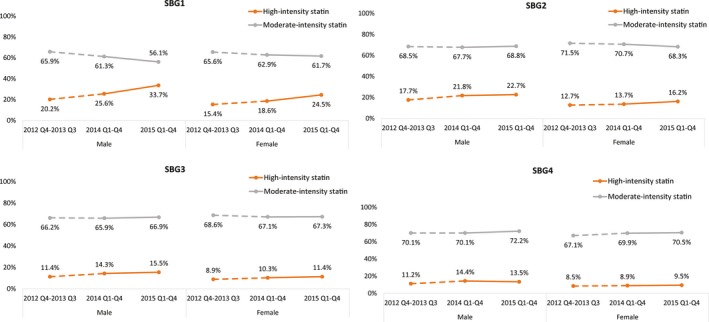
Methods and results: This retrospective, observational study used administrative medical and pharmacy claims data to identify patients newly initiated on statin therapy over 4 quarters prior to and 8 quarters following the release of the guideline (average N/quarter=3596). Patients were divided into the 4 statin benefit groups (SBGs) based on risk factors and laboratory lipid levels as defined in the guideline: SBG1 (with atherosclerotic cardiovascular disease [ASCVD]; N=1046/quarter), SBG2 (without ASCVD, with low-density lipoprotein cholesterol ≥190 mg/dL; N=454/quarter), SBG3 (without ASCVD, aged 40-75 years, with diabetes mellitus, low-density lipoprotein cholesterol 70-189 mg/dL; N=1391/quarter), SBG4 (no ASCVD or diabetes mellitus, age 40-75 years, low-density lipoprotein cholesterol 70-189 mg/dL, estimated 10-year ASCVD risk of ≥7.5%; N=705/quarter). Demographic variables, statin utilization patterns, lipid levels, and comorbidities were analyzed for pre- and postguideline periods. Postguideline, gradually increased high-intensity statin initiation occurred in SBG1, SBG2, and in SBG3 patients with 10-year ASCVD risk ≥7.5%. Moderate- to high-intensity statin initiation gradually increased among SBG4 patients. Recommended-intensity statin choice changed to a greater degree among patients treated by specialty care physicians. Regarding sex, target-intensity statin initiation was lower in women in all groups before and after guideline release.
Conclusions: Prescriber implementation of the guideline recommendations has gradually increased, with the most marked change in the increased initiation of high-intensity statins in patients with ASCVD and in those treated by a specialist.
Keywords: American College of Cardiology/American Heart Association; cholesterol; guidelines; lipids; statins.
© 2017 The Authors, AstraZeneca, and HealthCore. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures

References
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd‐Jones DM, McBride P, Schwartz JS, Shero ST, Smith JSC, Watson K, Wilson PWF. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2889–2934. - PubMed
-
- Johnson KM, Dowe DA. Accuracy of statin assignment using the 2013 AHA/ACC cholesterol guideline versus the 2001 NCEP ATP III guideline correlation with atherosclerotic plaque imaging. J Am Coll Cardiol. 2014;64:910–919. - PubMed
-
- Goff JDC, Lloyd‐Jones DM, Bennett G, Coady S, D'Agostino SRB, Gibbons R, Greenland P, Lackland DT, Levy D, O'Donnell CJ, Robinson JG, Schwartz JS, Shero ST, Smith JSC, Sorlie P, Stone NJ, Wilson PWF; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2935–2959. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
