

Central Positional Nystagmus: A Systematic Literature Review
- PMID: 28473800
- PMCID: PMC5397512
- DOI: 10.3389/fneur.2017.00141
Central Positional Nystagmus: A Systematic Literature Review
Abstract
Objective: To provide a systematic review of the clinical and radiological features of lesion-induced central positional nystagmus (CPN) and identify salient characteristics that differentiate central from peripheral positional nystagmus (PN).
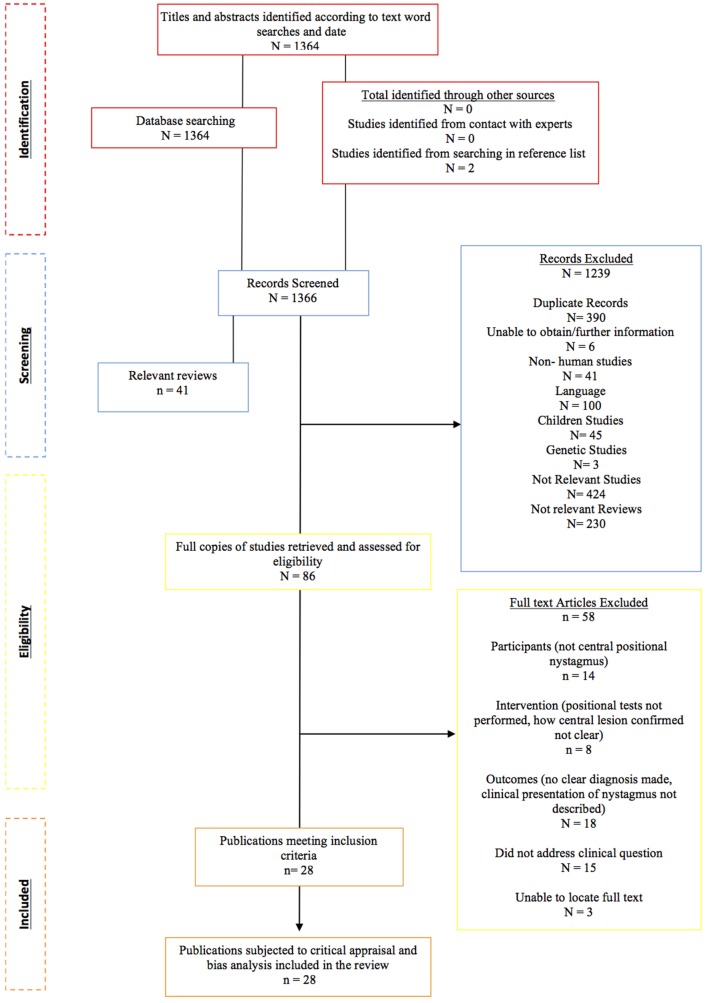
Methods: Systematic literature search according to the preferred reporting items for systematic reviews and meta-analysis.
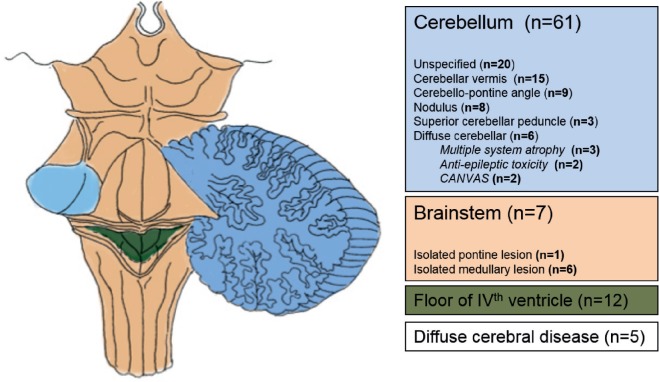
Results: A total of 82 patients from 28 studies met the participants intervention, comparison, outcomes, and study designs criteria for inclusion. An atypical direction of nystagmus for the stimulated canal was reported in 97.5% patients during Dix-Hallpike (D-H) and 54.5% upon supine roll testing. Five types of CPNs were identified during positional testing: positional horizontal nystagmus (pHN) (36.8%), positional downbeating nystagmus (pDBN) (29.2%), positional torsional nystagmus (pTN) (2.1%), positional upbeating nystagmus (pUBN) (2.1%), and a combination of the four profiles (29.9%). CPN was paroxysmal (<60 s) in 85% patients on straight head hanging (SHH), 63.9% on D-H, and 37.5% on supine roll, and had a latency <3 s upon positioning in 94.7% patients in which it was reported. Concurrent vertigo was reportedly present in 63.4% patients and 48.8% demonstrated other neurological signs. Radiologically, in 74.4%, there was mention of cerebellar involvement, isolated brainstem involvement in 8.5%, and 14.6% involved the fourth ventricle.
Conclusion: Currently, there is a lack of robust data on the clinical and radiological characteristics of CPN highlighting the need for better phenotyping of CPN to help differentiate this entity from peripheral causes of PN. With increased awareness of CPN, particularly in the acute setting, we may see a change in the estimated prevalence of CPN and improved clinical markers to promptly identify the frequently sinister underlying causes.
Keywords: central positional nystagmus; central positional vertigo; nystagmus; positional nystagmus; positional vertigo; vertigo.
Figures
Similar articles
-
Central positional nystagmus: an update.J Neurol. 2022 Apr;269(4):1851-1860. doi: 10.1007/s00415-021-10852-8. Epub 2021 Oct 20. J Neurol. 2022. PMID: 34669008 Review.
-
Central positional nystagmus: Characteristics and model-based explanations.Prog Brain Res. 2019;249:211-225. doi: 10.1016/bs.pbr.2019.04.012. Epub 2019 May 15. Prog Brain Res. 2019. PMID: 31325981
-
Anterior semicircular canal benign paroxysmal positional vertigo and positional downbeating nystagmus.Am J Otolaryngol. 2006 May-Jun;27(3):173-8. doi: 10.1016/j.amjoto.2005.09.010. Am J Otolaryngol. 2006. PMID: 16647981
-
[The exploration on optimization of two alternatives between roll test and Dix-Hallpike test in benign paroxysmal positional vertigo].Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017 Jun 7;52(6):440-445. doi: 10.3760/cma.j.issn.1673-0860.2017.06.009. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017. PMID: 28635217 Chinese.
-
Positional and positioning vertigo and nystagmus.J Neurol Sci. 1990 Jan;95(1):3-28. doi: 10.1016/0022-510x(90)90113-2. J Neurol Sci. 1990. PMID: 2187057 Review.
Cited by
-
Increased Risk of Neurodegenerative Dementia after Benign Paroxysmal Positional Vertigo.Int J Environ Res Public Health. 2021 Oct 8;18(19):10553. doi: 10.3390/ijerph181910553. Int J Environ Res Public Health. 2021. PMID: 34639856 Free PMC article.
-
Clinical spectrum of positional downbeat nystagmus: a diagnostic approach.J Neurol. 2025 Jan 23;272(2):163. doi: 10.1007/s00415-024-12883-3. J Neurol. 2025. PMID: 39849040 Review.
-
Detecting positional vertigo using an ensemble of 2D convolutional neural networks.Biomed Signal Process Control. 2021 Jul;68:102708. doi: 10.1016/j.bspc.2021.102708. Biomed Signal Process Control. 2021. PMID: 34276807 Free PMC article.
-
The clinical significance of direction-fixed mono-positional apogeotropic horizontal nystagmus.Acta Otorhinolaryngol Ital. 2022 Jun;42(3):287-292. doi: 10.14639/0392-100X-N1824. Acta Otorhinolaryngol Ital. 2022. PMID: 35880369 Free PMC article.
-
Diagnosing Stroke in Acute Dizziness and Vertigo: Pitfalls and Pearls.Stroke. 2018 Mar;49(3):788-795. doi: 10.1161/STROKEAHA.117.016979. Epub 2018 Feb 19. Stroke. 2018. PMID: 29459396 Free PMC article. Review. No abstract available.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous