

Recovery of Abnormal ABR in Neonates and Infants at Risk of Hearing Loss
- PMID: 28473856
- PMCID: PMC5394396
- DOI: 10.1155/2017/7912127
Recovery of Abnormal ABR in Neonates and Infants at Risk of Hearing Loss
Abstract
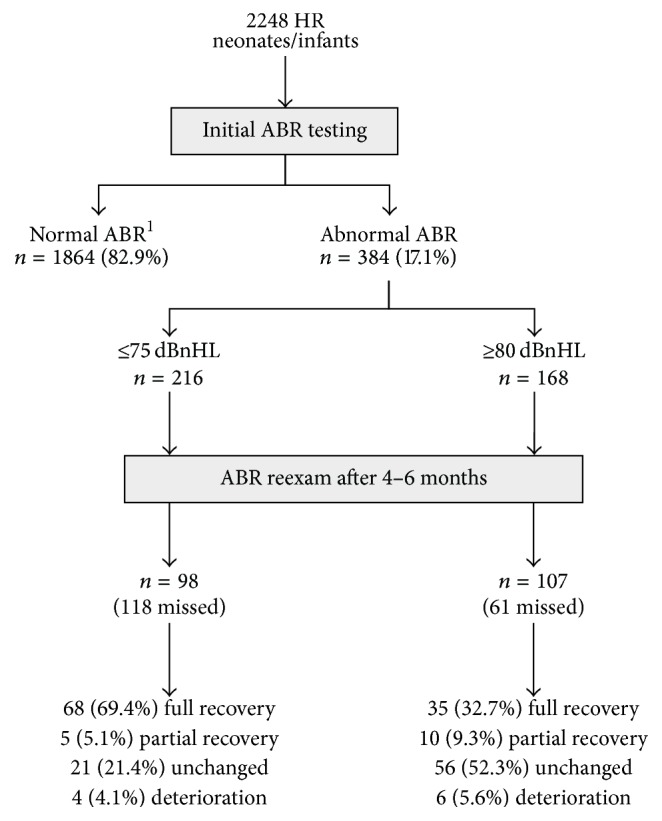
The purpose of this retrospective study is to present the clinical experience of a single institution on the recovery of ABR thresholds in a large population of neonates and infants at risk of hearing loss. Potential prognostic factors associated with this phenomenon were also investigated. Out of 2248 high risk infants, 384 had abnormal ABR at initial hearing evaluation and 168 of them had absent ABR or a threshold ≥80 dBnHL. From this subgroup, a significant percentage showed complete or partial recovery on reexamination (32.7% and 9.3%, resp.), performed 4-6 months later. The presence of normal otoacoustic emissions was associated with the ABR restoration on reexamination. Moreover, the very young age at the initial hearing screening seems to be related to higher probabilities of false positive ABR. The potential recovery of hearing in HR infants raises concerns about the very early cochlear implantation in HR infants less than one year. Such a treatment modality should be decided cautiously and only after obtaining valid and stable objective and subjective hearing thresholds. This holds especially true for infants showing an auditory neuropathy profile, as they presented a much greater probability of ABR recovery.
Figures
Similar articles
-
Transient infantile auditory neuropathy and its clinical implications.Int J Pediatr Otorhinolaryngol. 2006 Sep;70(9):1629-37. doi: 10.1016/j.ijporl.2006.05.005. Int J Pediatr Otorhinolaryngol. 2006. PMID: 16769129
-
Reversible auditory brainstem responses screening failures in high risk neonates.Eur Arch Otorhinolaryngol. 2011 Feb;268(2):189-96. doi: 10.1007/s00405-010-1363-3. Epub 2010 Aug 15. Eur Arch Otorhinolaryngol. 2011. PMID: 20711783
-
Early detection of neonatal hearing loss by otoacoustic emissions and auditory brainstem response over 10 years of experience.Int J Pediatr Otorhinolaryngol. 2019 Dec;127:109647. doi: 10.1016/j.ijporl.2019.109647. Epub 2019 Aug 21. Int J Pediatr Otorhinolaryngol. 2019. PMID: 31470205
-
Association of Audiometric Measures with plasma long chain polyunsaturated fatty acids in a high-fish eating population: The Seychelles Child Development Study.Neurotoxicology. 2020 Mar;77:137-144. doi: 10.1016/j.neuro.2020.01.005. Epub 2020 Jan 23. Neurotoxicology. 2020. PMID: 31982419 Free PMC article. Review.
-
Clinicians' Guide to Obtaining a Valid Auditory Brainstem Response to Determine Hearing Status: Signal, Noise, and Cross-Checks.Am J Audiol. 2018 Mar 8;27(1):25-36. doi: 10.1044/2017_AJA-17-0074. Am J Audiol. 2018. PMID: 29392291 Review.
Cited by
-
Isolated auditory neuropathy at birth in congenital cytomegalovirus infection.Ital J Pediatr. 2020 Jan 6;46(1):3. doi: 10.1186/s13052-019-0767-y. Ital J Pediatr. 2020. PMID: 31906974 Free PMC article.
-
Comparing Auditory Brain Stem Responses and Transient Otoacoustic Emissions in Premature Infants with Auditory Developmental Delay: Evidence of Temporary Auditory Neuropathy.Iran J Child Neurol. 2023 Fall;17(4):35-44. doi: 10.22037/ijcn.v17i4.42882. Epub 2023 Oct 26. Iran J Child Neurol. 2023. PMID: 38074936 Free PMC article.
-
Prevalence of permanent childhood hearing loss detected at the universal newborn hearing screen: Systematic review and meta-analysis.PLoS One. 2019 Jul 11;14(7):e0219600. doi: 10.1371/journal.pone.0219600. eCollection 2019. PLoS One. 2019. PMID: 31295316 Free PMC article.
-
Neuronal development in the cochlea of a nonhuman primate model, the common marmoset.Dev Neurobiol. 2021 Nov;81(8):905-938. doi: 10.1002/dneu.22850. Epub 2021 Oct 22. Dev Neurobiol. 2021. PMID: 34545999 Free PMC article.
References
-
- Perlman M., Fainmesser P., Sohmer H., Tamari H., Wax Y., Pevsmer B. Auditory nerve-brainstem evoked responses in hyperbilirubinemic neonates. Pediatrics. 1983;72(5):658–664. - PubMed
-
- Nwaesei C. G., Van Aerde J., Boyden M., Perlman M. Changes in auditory brainstem responses in hyperbilirubinemic infants before and after exchange transfusion. Pediatrics. 1984;74(5):800–803. - PubMed
-
- Nakamura H., Takada S., Shimabuku R., Matsuo M., Matsuo T., Negishi H. Auditory nerve and brainstem responses in newborn infants with hyperbilirubinemia. Pediatrics. 1985;75(4):703–708. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
