

A review and critical appraisal of central axis flaps in axillary and elbow contractures
- PMID: 28473994
- PMCID: PMC5415992
- DOI: 10.1186/s41038-017-0079-7
A review and critical appraisal of central axis flaps in axillary and elbow contractures
Abstract
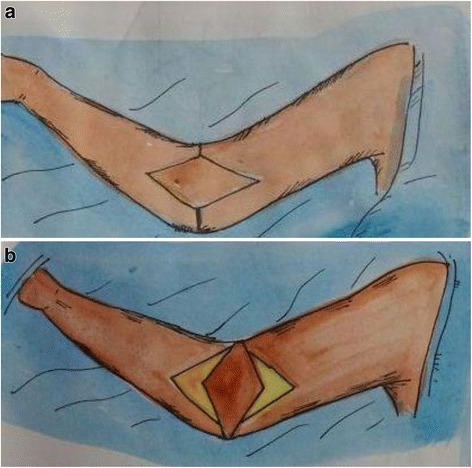
Contractures of the axilla and elbow can produce a significant impact on quality of life by reducing the ability to perform activities of daily living. Varieties of techniques are available for resurfacing defects following contracture release but graft or flap loss, donor-site morbidity, esthetics, and recurrences are still challenges for reconstructive surgeons. Central axis "propeller" flaps based on a random, subcutaneous pedicle were first described for axillary and elbow contractures to deploy the unburnt skin of axillary dome in type I and II contractures (Kurtzman and Stern) by moving them 90° to straddle the contracting bands. This strategy provided better esthetics and avoided prolonged splinting. Over more than two decades, there have been several design modifications of these flaps with extended applications to cubital fossa. A comprehensive review of published literature on the topic is presented to discuss classifications, design modifications, and applications of such flaps in managing axillary and elbow contractures.
Keywords: Axillary contracture; Central axis flap; Elbow contracture; Propeller flap; Subcutaneous pedicled flap.
Figures








References
-
- Huang T, Yang JY. Management of contractural deformities involving the shoulder (axilla), elbow, hip and knee joints in burned patients. In: Herndon DN, editor. Total burn Care. 4. Philadelphia: Elsevier; 2012.
-
- Salam GA, Amin JP. The basic Z-plasty. Am Fam Physician. 2003;67:2329–2332. - PubMed
-
- Hyakusoku H, Shirai H, Umeda T, Fumiiri M. The use of the square flap method for repair of axillary burn contracture. Plast Reconstr Surg. 1985;28:585.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
