

Dabrafenib plus trametinib versus dabrafenib monotherapy in patients with metastatic BRAF V600E/K-mutant melanoma: long-term survival and safety analysis of a phase 3 study
- PMID: 28475671
- PMCID: PMC5834102
- DOI: 10.1093/annonc/mdx176
Dabrafenib plus trametinib versus dabrafenib monotherapy in patients with metastatic BRAF V600E/K-mutant melanoma: long-term survival and safety analysis of a phase 3 study
Erratum in
-
Dabrafenib plus trametinib versus dabrafenib monotherapy in patients with metastatic BRAF V600E/K-mutant melanoma: long-term survival and safety analysis of a phase 3 study.Ann Oncol. 2019 Nov 1;30(11):1848. doi: 10.1093/annonc/mdz221. Ann Oncol. 2019. PMID: 31406976 Free PMC article. No abstract available.
Abstract
Background: Previous analysis of COMBI-d (NCT01584648) demonstrated improved progression-free survival (PFS) and overall survival (OS) with combination dabrafenib and trametinib versus dabrafenib monotherapy in BRAF V600E/K-mutant metastatic melanoma. This study was continued to assess 3-year landmark efficacy and safety after ≥36-month follow-up for all living patients.
Patients and methods: This double-blind, phase 3 study enrolled previously untreated patients with BRAF V600E/K-mutant unresectable stage IIIC or stage IV melanoma. Patients were randomized to receive dabrafenib (150 mg twice daily) plus trametinib (2 mg once daily) or dabrafenib plus placebo. The primary endpoint was PFS; secondary endpoints were OS, overall response, duration of response, safety, and pharmacokinetics.
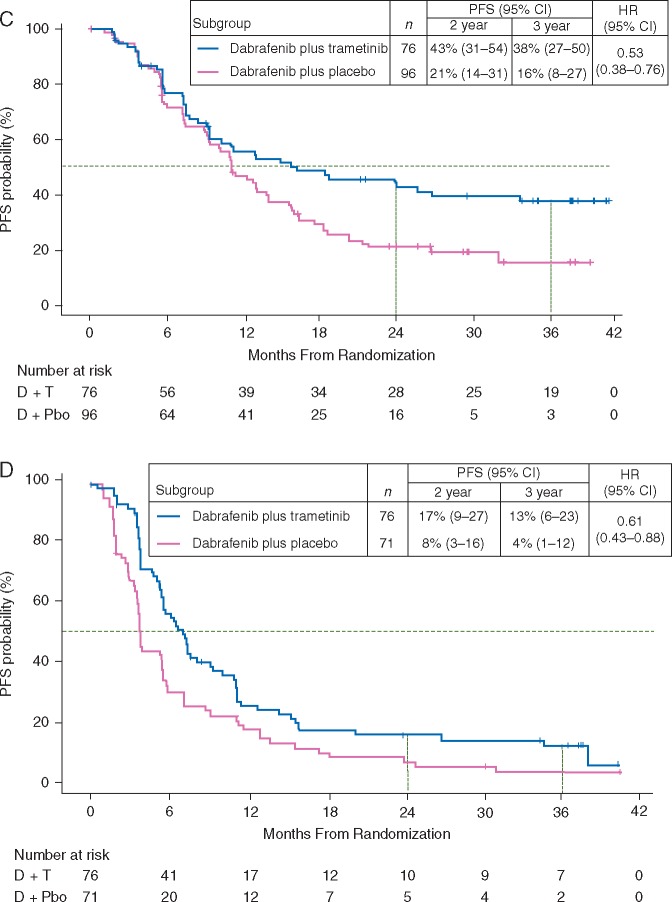
Results: Between 4 May and 30 November 2012, a total of 423 of 947 screened patients were randomly assigned to receive dabrafenib plus trametinib (n = 211) or dabrafenib monotherapy (n = 212). At data cut-off (15 February 2016), outcomes remained superior with the combination: 3-year PFS was 22% with dabrafenib plus trametinib versus 12% with monotherapy, and 3-year OS was 44% versus 32%, respectively. Twenty-five patients receiving monotherapy crossed over to combination therapy, with continued follow-up under the monotherapy arm (per intent-to-treat principle). Of combination-arm patients alive at 3 years, 58% remained on dabrafenib plus trametinib. Three-year OS with the combination reached 62% in the most favourable subgroup (normal lactate dehydrogenase and <3 organ sites with metastasis) versus only 25% in the unfavourable subgroup (elevated lactate dehydrogenase). The dabrafenib plus trametinib safety profile was consistent with previous clinical trial observations, and no new safety signals were detected with long-term use.
Conclusions: These data demonstrate that durable (≥3 years) survival is achievable with dabrafenib plus trametinib in patients with BRAF V600-mutant metastatic melanoma and support long-term first-line use of the combination in this setting.
Keywords: BRAF; dabrafenib; durable outcomes; melanoma; metastatic; trametinib.
© The Author 2017. Published by Oxford University Press on behalf of the European Society for Medical Oncology.
Figures



References
-
- Barth A, Wanek LA, Morton DL.. Prognostic factors in 1,521 melanoma patients with distant metastases. J Am Coll Surg 1995; 181: 193–201. - PubMed
-
- Long GV, Stroyakovskiy D, Gogas H. et al. Dabrafenib and trametinib versus dabrafenib and placebo for Val600 BRAF-mutant melanoma: a multicentre, double-blind, phase 3 randomised controlled trial. Lancet 2015; 386: 444–451. - PubMed
-
- Robert C, Karaszewska B, Schachter J. et al. Two year estimate of overall survival in COMBI-v, a randomized, open-label, phase III study comparing the combination of dabrafenib (D) and trametinib (T) with vemurafenib (Vem) as first-line therapy in patients (pts) with unresectable or metastatic BRAF V600E/K mutation-positive cutaneous melanoma. Eur J Cancer 2015; 51(Suppl. 3): S663, abstr 3301.
-
- Ascierto PA, McArthur GA, Dreno B. et al. Cobimetinib combined with vemurafenib in advanced BRAFV600-mutant melanoma (coBRIM): updated efficacy results from a randomised, double-blind, phase 3 trial. Lancet Oncol 2016; 17: 1248–1260. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
