

Matrix Degradation in Human Immunodeficiency Virus Type 1-Associated Tuberculosis and Tuberculosis Immune Reconstitution Inflammatory Syndrome: A Prospective Observational Study
- PMID: 28475709
- PMCID: PMC5815569
- DOI: 10.1093/cid/cix231
Matrix Degradation in Human Immunodeficiency Virus Type 1-Associated Tuberculosis and Tuberculosis Immune Reconstitution Inflammatory Syndrome: A Prospective Observational Study
Abstract
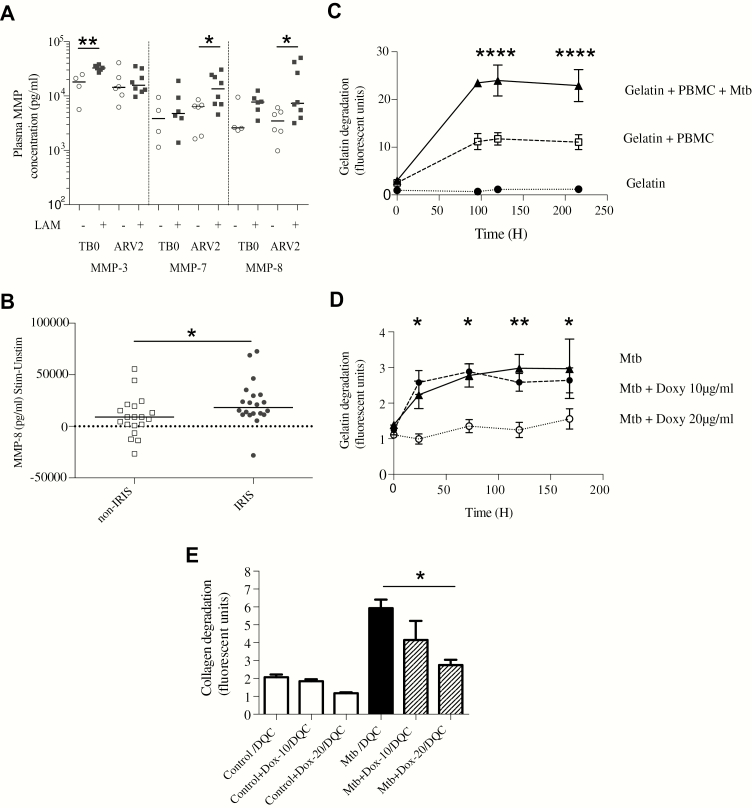
Background: Extensive immunopathology occurs in human immunodeficiency virus (HIV)/tuberculosis (TB) coinfection, but the underlying molecular mechanisms are not well-defined. Excessive matrix metalloproteinase (MMP) activity is emerging as a key process but has not been systematically studied in HIV-associated TB.
Methods: We performed a cross-sectional study of matrix turnover in HIV type 1 (HIV-1)-infected and -uninfected TB patients and controls, and a prospective cohort study of HIV-1-infected TB patients at risk of TB immune reconstitution inflammatory syndrome (TB-IRIS), in Cape Town, South Africa. Sputum and plasma MMP concentrations were quantified by Luminex, plasma procollagen III N-terminal propeptide (PIIINP) by enzyme-linked immunosorbent assay, and urinary lipoarabinomannan (LAM) by Alere Determine TB LAM assay. Peripheral blood mononuclear cells from healthy donors were cultured with Mycobacterium tuberculosis and extracellular matrix in a 3D model of TB granuloma formation.
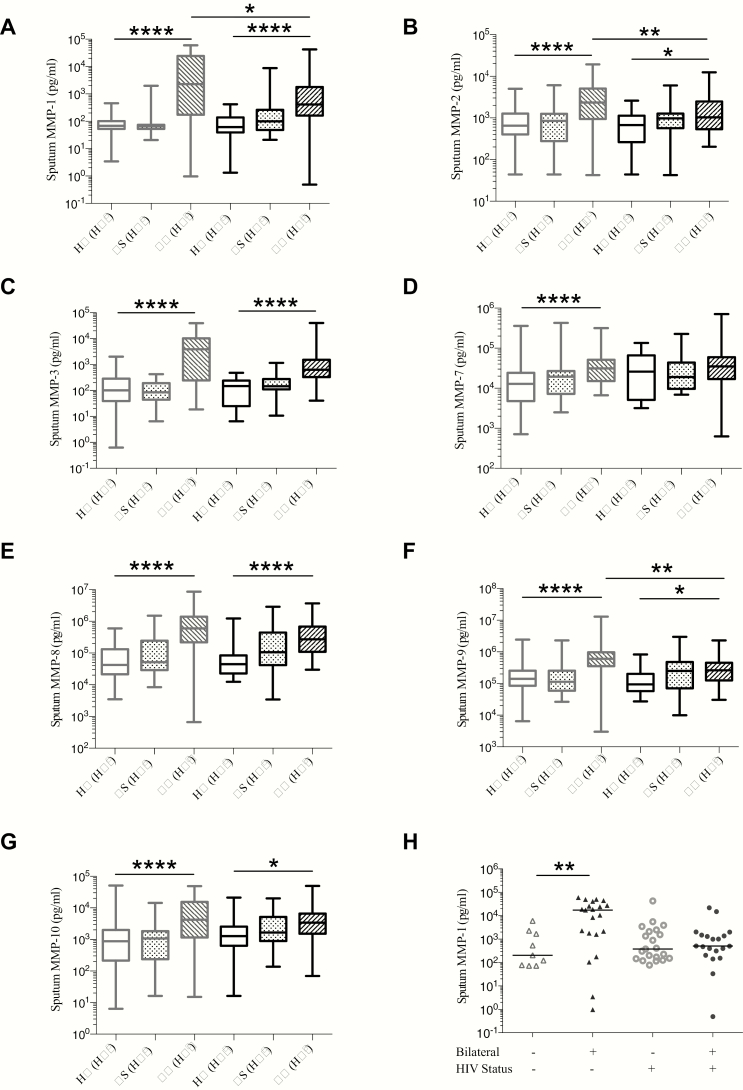
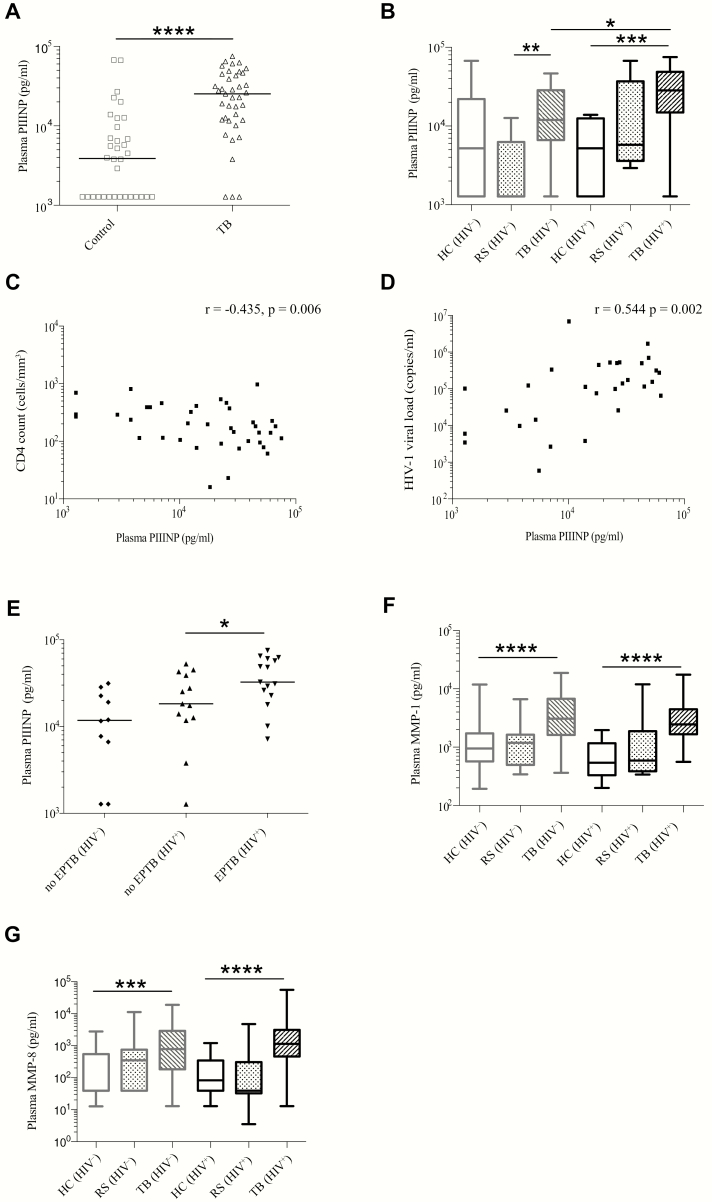
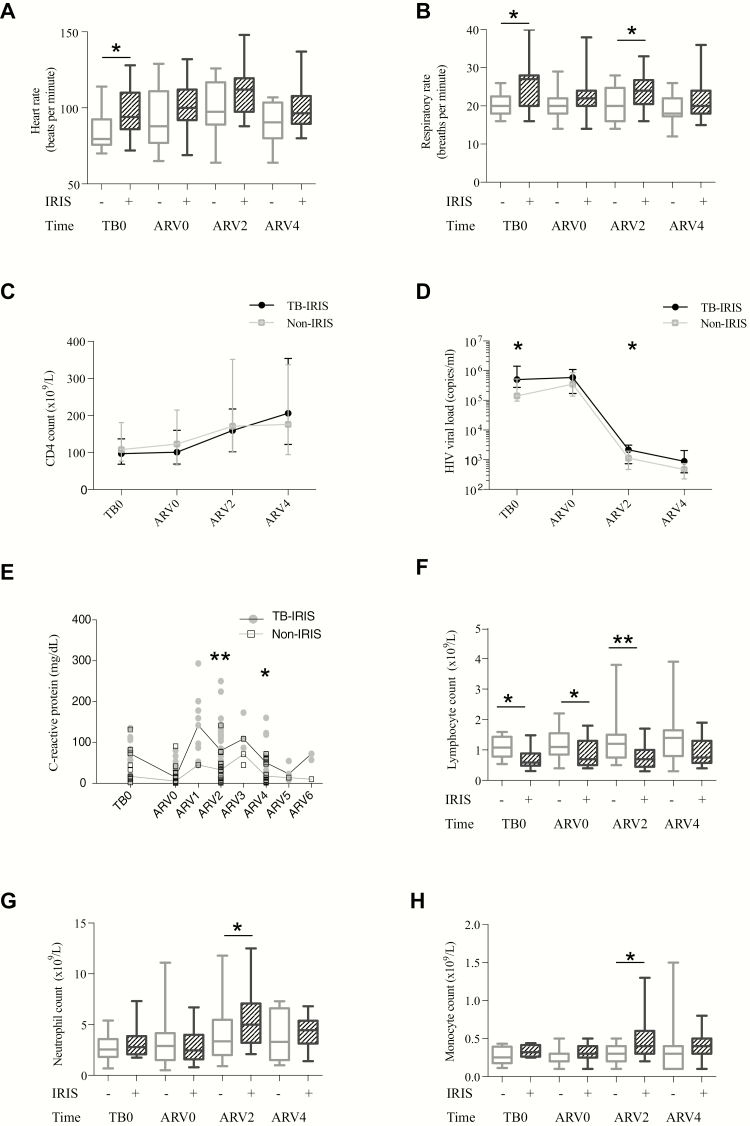
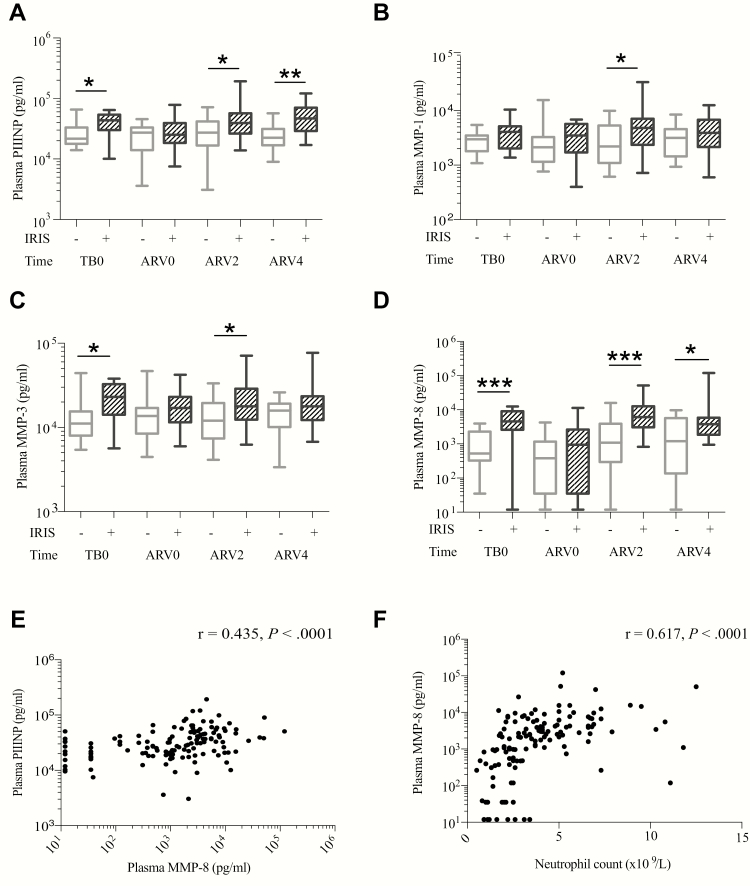
Results: MMP activity differed between HIV-1-infected and -uninfected TB patients and corresponded with specific TB clinical phenotypes. HIV-1-infected TB patients had reduced pulmonary MMP concentrations, associated with reduced cavitation, but increased plasma PIIINP, compared to HIV-1-uninfected TB patients. Elevated extrapulmonary extracellular matrix turnover was associated with TB-IRIS, both before and during TB-IRIS onset. The predominant collagenase was MMP-8, which was likely neutrophil derived and M. tuberculosis-antigen driven. Mycobacterium tuberculosis-induced matrix degradation was suppressed by the MMP inhibitor doxycycline in vitro.
Conclusions: MMP activity in TB differs by HIV-1 status and compartment, and releases matrix degradation products. Matrix turnover in HIV-1-infected patients is increased before and during TB-IRIS, informing novel diagnostic strategies. MMP inhibition is a potential host-directed therapy strategy for prevention and treatment of TB-IRIS.
Keywords: HIV-1; immune reconstitution inflammatory syndrome; matrix metalloproteinase; procollagen III N-terminal propeptide; tuberculosis.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
