

Comparing Drivers and Dynamics of Tuberculosis in California, Florida, New York, and Texas
- PMID: 28475845
- PMCID: PMC5808932
- DOI: 10.1164/rccm.201702-0377OC
Comparing Drivers and Dynamics of Tuberculosis in California, Florida, New York, and Texas
Abstract
Rationale: There is substantial state-to-state heterogeneity in tuberculosis (TB) in the United States; better understanding this heterogeneity can inform effective response to TB at the state level, the level at which most TB control efforts are coordinated.
Objectives: To characterize drivers of state-level heterogeneity in TB epidemiology in the four U.S. states that bear half the country's TB burden: California, Florida, New York, and Texas.
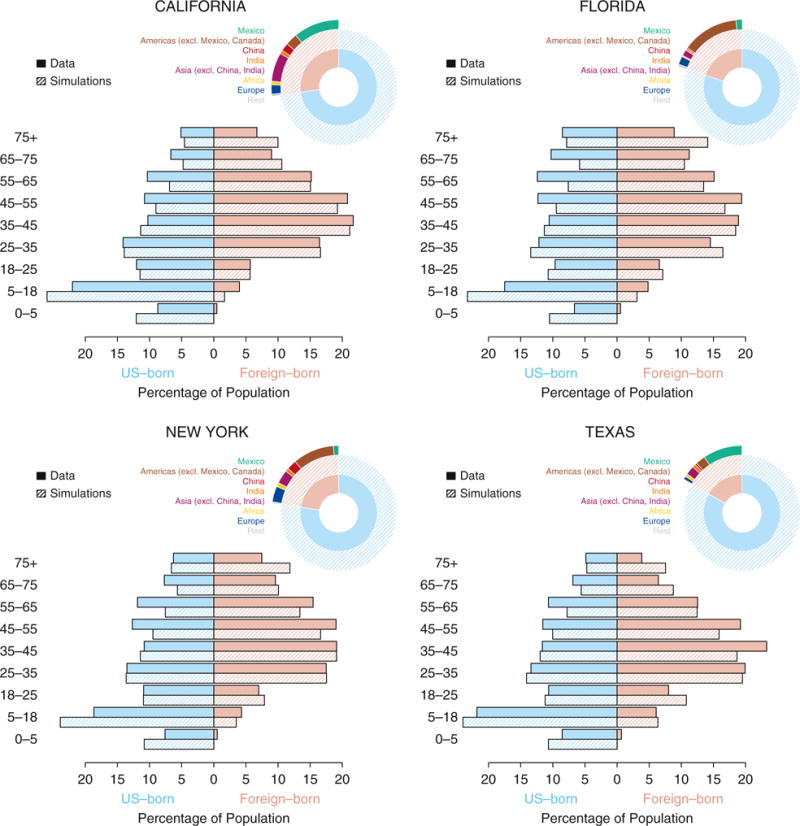
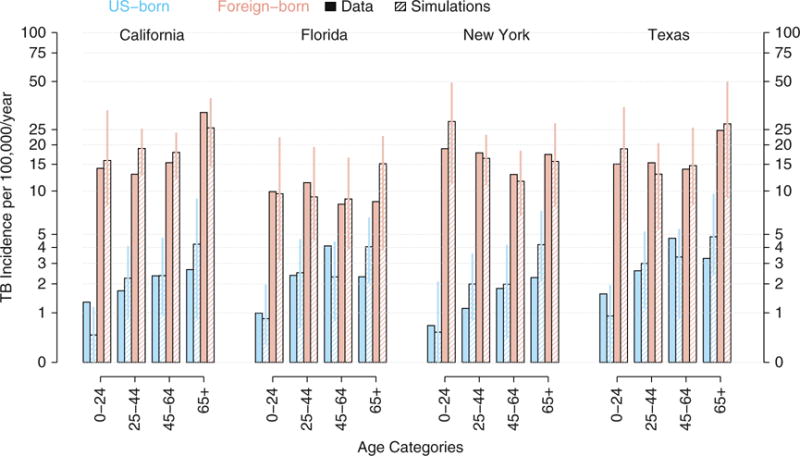
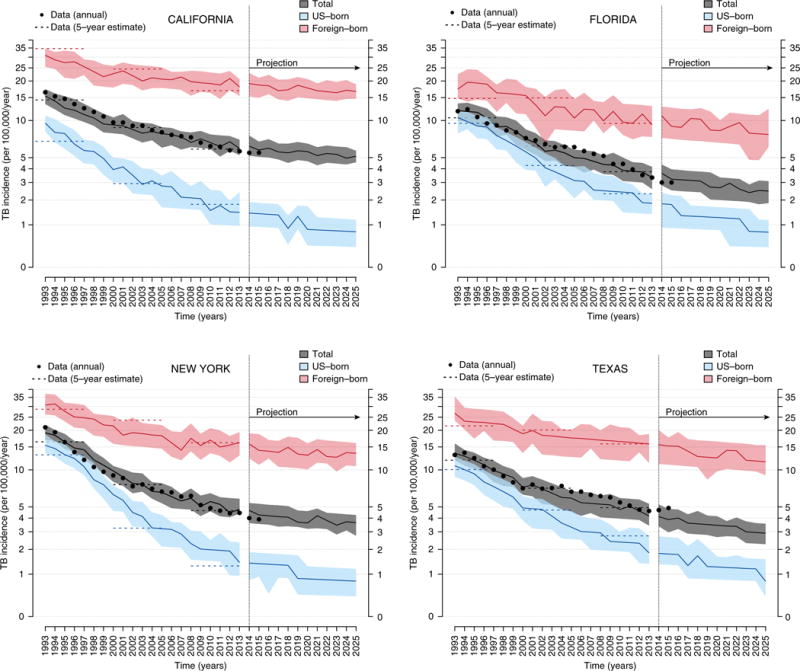
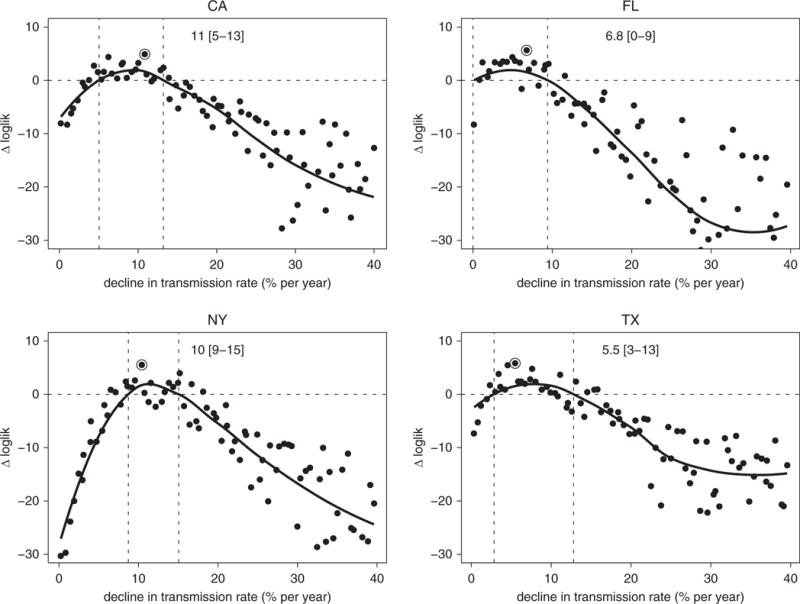
Methods: We constructed an individual-based model of TB in the four U.S. states and calibrated the model to state-specific demographic and age- and nativity-stratified TB incidence data. We used the model to infer differences in natural history of TB and in future projections of TB.
Measurements and main results: We found that differences in both demographic makeup (particularly the size and composition of the foreign-born population) and TB transmission dynamics contribute to state-level differences in TB epidemiology. The projected median annual rate of decline in TB incidence in the next decade was substantially higher in Texas (3.3%; 95% range, -5.6 to 10.9) than in California (1.7%; 95% range, -3.8 to 7.1), Florida (1.5%; 95% range, -7.4 to 14), and New York (1.9%; 95% range, -6.4 to 9.8). All scenarios projected a flattening of the decline in TB incidence by 2025 without additional resources or interventions.
Conclusions: There is substantial state-level heterogeneity in TB epidemiology in the four states, which reflect both demographic factors and potential differences in the natural history of TB. These differences may inform resource allocation decisions in these states.
Keywords: geographical heterogeneity in tuberculosis; mathematical modeling of tuberculosis; tuberculosis; tuberculosis in the United States.
Figures

Comment in
-
The Use of Modeling to Compare Tuberculosis Dynamics in Four U.S. States.Am J Respir Crit Care Med. 2017 Oct 15;196(8):953-954. doi: 10.1164/rccm.201705-0963ED. Am J Respir Crit Care Med. 2017. PMID: 28609634 No abstract available.
References
-
- Centers for Disease Control and Prevention. Reported tuberculosis in the United States, 2015. Atlanta, GA: U.S. Department of Health and Human Services, CDC; 2016.
-
- Salinas JL, Mindra G, Haddad MB, Pratt R, Price SF, Langer AJ. Leveling of tuberculosis incidence - United States, 2013-2015. MMWR Morb Mortal Wkly Rep. 2016;65:273–278. - PubMed
-
- Pew Research Center. Statistical portrait of the foreign-born population in the United States. 2016 Apr 19; [accessed 2017 Aug 2]. Available from: http://www.pewhispanic.org/2016/04/19/statistical-portrait-of-the-foreig...
-
- Hill AN, Becerra J, Castro KG. Modelling tuberculosis trends in the USA. Epidemiol Infect. 2012;140:1862–1872. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
