

The combination of prostate imaging reporting and data system version 2 (PI-RADS v2) and periprostatic fat thickness on multi-parametric MRI to predict the presence of prostate cancer
- PMID: 28476042
- PMCID: PMC5546460
- DOI: 10.18632/oncotarget.17182
The combination of prostate imaging reporting and data system version 2 (PI-RADS v2) and periprostatic fat thickness on multi-parametric MRI to predict the presence of prostate cancer
Abstract
Purpose: To evaluate the auxiliary effectiveness of periprostatic fat thickness (PPFT) on multi-parametric magnetic resonance imaging (mp-MRI) to Prostate Imaging Reporting and Data System version 2 (PI-RADS v2) in predicting the presence of prostate cancer (PCa) and high-grade prostate cancer (HGPCa, Gleason Score ≥ 7).
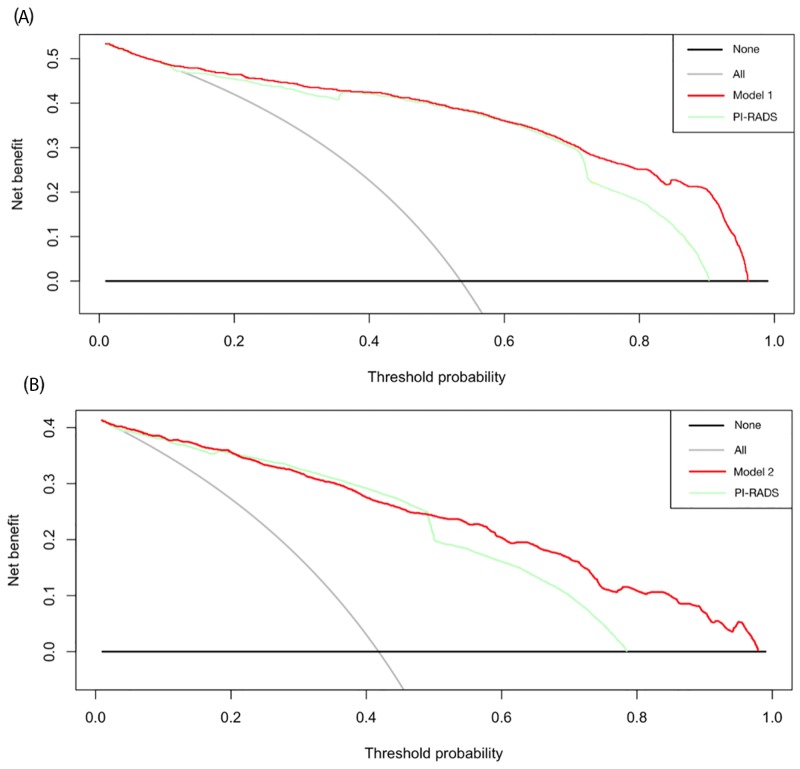
Results: Overall, there were 371 patients (54.3%) with PCa and 292 patients (42.8%) with HGPCa. The mean value of PPFT was 4.04 mm. Multivariate analysis revealed that age, prostatic specific antigen (PSA), volume, PI-RADS score, and PPFT were independent predictors of PCa. All factors plus abnormal digital rectal exam were independent predictors of HGPCa. In addition, the PPFT was the independent predictor of PCa (Odds ratio [OR] 2.56, p = 0.004) and HGPCa (OR 2.70, p = 0.014) for subjects with PI-RADS grade 3. The present two nomograms based on multivariate analysis outperformed the single PI-RADS in aspects of predicting accuracy for PCa (area under the curve: 0.922 vs. 0.883, p = 0.029) and HGPCa (0.919 vs. 0.873, p = 0.007). Decision-curve analysis also indicated the favorable clinical utility of the present two nomograms.
Materials and methods: The clinical data of 683 patients who received transrectal ultrasound guided biopsy and prior mp-MRI were reviewed. PPFT was measured as the shortest perpendicular distance from the pubic symphysis to the prostate on MRI. Univariate and multivariate analyses were performed to determine the independent predictors of PCa and HGPCa. We also constructed two nomograms for predicting PCa and HGPCa based on the logistic regression.
Conclusion: The PPFT on mp-MRI is an independent predictor of PCa and HGPCa, notably for patients with PI-RADS grade 3. The nomograms incorporated predictors of PPFT and PI-RADS demonstrated good predictive performance.
Keywords: PI-RADS; diagnosis; nomogram; periprostatic fat; prostate cancer.
Conflict of interest statement
The authors of this article have no conflicts of interest.
Figures



References
-
- Heidenreich A, Bastian PJ, Bellmunt J, Bolla M, Joniau S, van der Kwast T, Mason M, Matveev V, Wiegel T, Zattoni F, Mottet N. European Association of U. EAU guidelines on prostate cancer. part 1: screening, diagnosis, and local treatment with curative intent-update 2013. Eur Urol. 2014;65:124–37. doi: 10.1016/j.eururo.2013.09.046. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
