

The Timed Up and Go Test as a Measure of Frailty in Urologic Practice
- PMID: 28477941
- PMCID: PMC5522780
- DOI: 10.1016/j.urology.2017.03.054
The Timed Up and Go Test as a Measure of Frailty in Urologic Practice
Abstract
Objective: To evaluate the prevalence of frailty, a known predictor of poor outcomes, among patients presenting to an academic nononcologic urology practice and to examine whether frailty differs among patients who did and did not undergo urologic surgery.
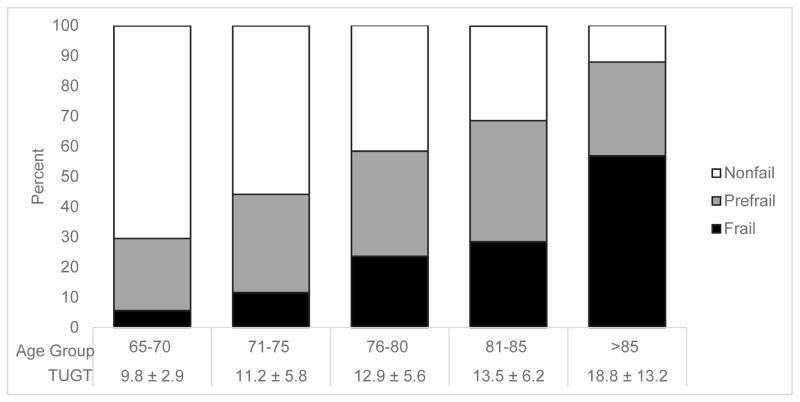
Methods: The Timed Up and Go Test (TUGT), a parsimonious measure of frailty, was administered to patients ages ≥65. The TUGT, demographic data, urologic diagnoses, and procedural history were abstracted from the medical record into a prospective database. TUGT times were categorized as nonfrail (≤10 seconds), prefrail (11-14 seconds), and frail (≥15 seconds). These times were evaluated across age and urologic diagnoses and compared between patients who did and did not undergo urologic surgery using chi-square and t tests.
Results: The TUGT was recorded for 78.9% of patient visits from December 2015 to May 2016. For 1089 patients, average age was 73.3 ± 6.3 years; average TUGT time was 11.6 ± 6.0 seconds; 30.0% were categorized as prefrail and 15.2% as frail. TUGT times increased with age, with 56.9% of patients age 86 and over categorized as frail. Times varied across diagnoses (highest average TUGT was 14.3 ± 11.9 seconds for patients with urinary tract infections); however, no difference existed between patients who did and did not undergo surgery (P = .94).
Conclusion: Among our population, prefrailty and frailty were common, TUGT times increased with age and varied by urologic diagnosis, but did not differ between patients who did and did not undergo urologic surgery, presenting an opportunity to consider frailty in preoperative surgical decision making.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures

Comment in
-
Editorial Comment.Urology. 2017 Aug;106:37. doi: 10.1016/j.urology.2017.03.055. Epub 2017 Jun 1. Urology. 2017. PMID: 28579214 No abstract available.
References
-
- Drach GW, Griebling TL. Geriatric urology. Journal of the American Geriatrics Society. 2003 Jul;51(7 Suppl):S355–358. - PubMed
-
- Togoni P, Simonato A, Robutti N, et al. Preoperative risk factors for postoperative delirium (POD) after urological surgery in the elderly. Archives of gerontology and geriatrics. 2011 May-Jun;52(3):e166–169. - PubMed
-
- Bjurlin MA, Goble SM, Fantus RJ, Hollowell CM. Outcomes in geriatric genitourinary trauma. Journal of the American College of Surgeons. 2011 Sep;213(3):415–421. - PubMed
-
- Townsend NT, Robinson TN. Surgical Risk and Comorbidity in Older Urologic Patients. Clinics in geriatric medicine. 2015 Nov;31(4):591–601. - PubMed
-
- Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. The journals of gerontology. Series A, Biological sciences and medical sciences. 2001 Mar;56(3):M146–156. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
