

Statin Use and Risk of Cirrhosis and Related Complications in Patients With Chronic Liver Diseases: A Systematic Review and Meta-analysis
- PMID: 28479502
- PMCID: PMC5605397
- DOI: 10.1016/j.cgh.2017.04.039
Statin Use and Risk of Cirrhosis and Related Complications in Patients With Chronic Liver Diseases: A Systematic Review and Meta-analysis
Abstract
Background & aims: Statins have been variably shown to decrease risk and complications of chronic liver diseases (CLDs). We performed a systematic review and meta-analysis to evaluate the association between statins and risk of cirrhosis and related complications in patients with CLDs.
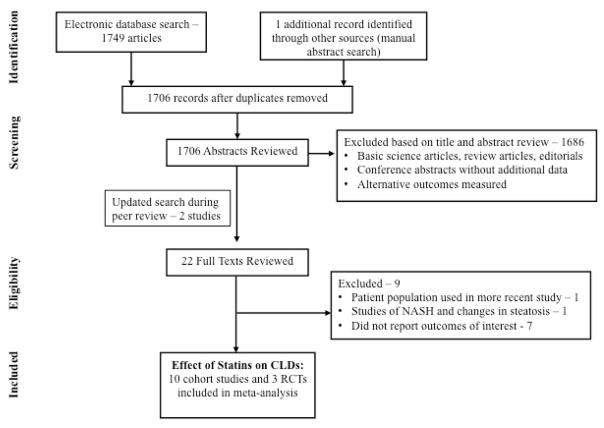
Methods: Through a systematic literature search up to March 2017, we identified 13 studies (3 randomized trials, 10 cohort studies) in adults with CLDs, reporting the association between statin use and risk of development of cirrhosis, decompensated cirrhosis, improvements in portal hypertension, or mortality. Pooled relative risk (RR) estimates with 95% confidence interval (CIs) were calculated using random effects model. Grading of Recommendations Assessment, Development and Evaluation criteria were used to assess quality of evidence.
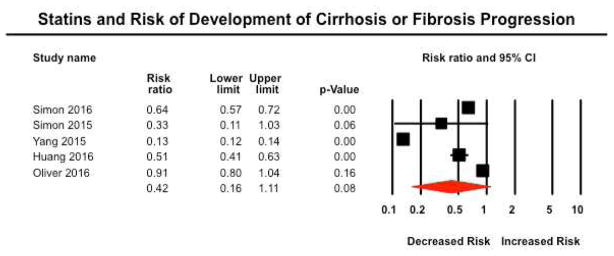
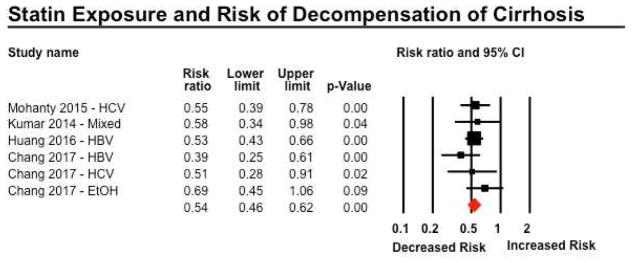
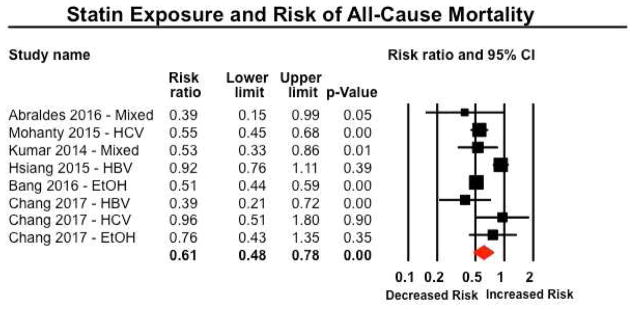
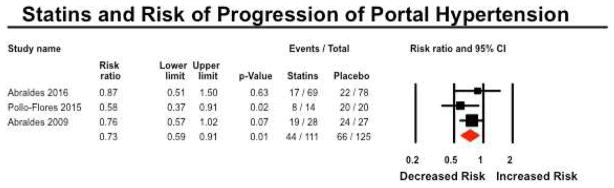
Results: Among 121,058 patients with CLDs (84.5% with hepatitis C), 46% were exposed to statins. In patients with cirrhosis, statin use was associated with 46% lower risk of hepatic decompensation (4 studies; RR, 0.54; 95% CI, 0.46-0.62; I2 = 0%; moderate-quality evidence), and 46% lower mortality (5 studies; RR, 0.54; 95% CI, 0.47-0.61; I2 = 10%; moderate-quality evidence). In patients with CLD without cirrhosis, statin use was associated with a nonsignificant (58% lower) risk of development of cirrhosis or fibrosis progression (5 studies; RR, 0.42; 95% CI, 0.16-1.11; I2 = 99%; very-low-quality evidence). In 3 randomized controlled trials, statin use was associated with 27% lower risk of variceal bleeding or progression of portal hypertension (hazard ratio, 0.73; 95% CI, 0.59-0.91; I2 = 0%; moderate-quality evidence).
Conclusions: Based on a systematic review and meta-analysis, statin use is probably associated with lower risk of hepatic decompensation and mortality, and might reduce portal hypertension, in patients with CLDs. Prospective observational studies and randomized controlled trials are needed to confirm this observation.
Keywords: Cholesterol-lowering Drug; Cirrhosis; Liver Fibrosis; Meta-analysis; RCT.
Copyright © 2017 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Xu J, Murphy SL, Kochanek KD, et al. Deaths: Final Data for 2013. National Vital Statistics Reports. 2016;64:1–119. - PubMed
-
- Grundy SM. HMG-CoA Reductase Inhibitors for Treatment of Hypercholesterolemia. N Engl J Med. 1988;319:24–33. - PubMed
-
- Endo A, MK, Tanzawa K. Competitive inhibition of 3-hydroxy-3-methylglutaryl coenzyme A reductase by ML-236A and ML-236B fungal metabolites, having hypocholesterolemic activity. FEBS Lett. 1976;1976:323–326. - PubMed
-
- Tsujita Y, Kuroda M, Tanzawa K, et al. Hypolipidemic effects in dogs of ML-236B, a competitive inhibitor of 3-hydroxy-3-methylglutaryl coenzyme A reductase. Atherosclerosis. 1979;32:307–313. - PubMed
-
- Shigematsu H, Hata Y, Yamamoto M, et al. Treatment of hypercholesterolemia with a HMG CoA reductase inhibitor (CS-500). I. Phase I study in normal subjects. Geriatr Med. 1979;17:1564–1570.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
