

Case Reports
doi: 10.4103/0976-3147.203831.
Cavernous Carotid Aneurysms: To Do or Not To Do?
Affiliations
- PMID: 28479810
- PMCID: PMC5402502
- DOI: 10.4103/0976-3147.203831
Item in Clipboard
Case Reports
Cavernous Carotid Aneurysms: To Do or Not To Do?
J Neurosci Rural Pract.
2017 Apr-Jun.
Abstract
Cavernous carotid aneurysms (CCA) pose considerable dilemmas in management. It is still unclear as to whether an asymptomatic CCA should be subjected to treatment. Similarly, the ideal management strategy for a symptomatic aneurysm is controversial. We present the case of a 60-year-old female with a giant CCA and discuss the management issues.
Keywords: Cavernous carotid aneurysms; cerebral bypass; unruptured aneurysms.
Conflict of interest statement
There are no conflicts of interest.
Figures

Magnetic resonance imaging (MRI) revealed a well defined extra axial altered signal intensity lesion measuring 4.0 x 4.1 x 3.4 cm in the left parasellar region which was heterogenous on T2W/FLAIR (a and c) iso to hyperintense on T1WI (b), and did not show any diffusion restriction. On post contrast (d) studies the central portion of the lesion showed homogenous intense enhancement while rest of the lesion did not show enhancement
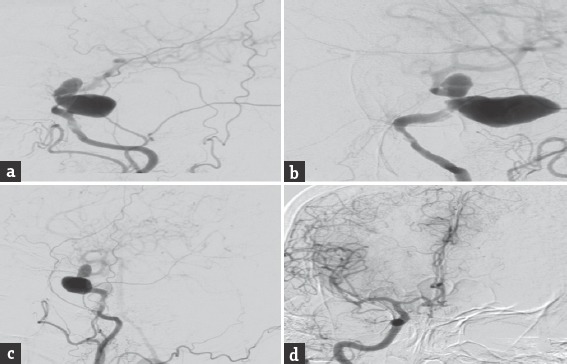
Digital subtraction angiography anteroposterior, lateral and oblique images (a-c) revealed a giant cavernous aneurysms measuring nearly 3.5 cm × 2.4 cm with areas of thrombosis. The aneurysm was seen extending superiorly into the intradural subarachnoid compartment. Cross circulation studies following compression of the left carotid artery revealed inadequate filling of the ipsilateral middle cerebral vessels (d)

Postoperative computed tomography angiogram revealed complete thrombosis of the aneurysm with no evidence of contrast enhancement. (c) The bypass graft showed normal contrast opacification (a and b) and there was no flow detected in the internal carotid artery distal to the occlusion (c)
Similar articles
-
Occipital lobe infarction: a rare presentation of bilateral giant cavernous carotid aneurysms: a case report.BMC Ophthalmol. 2018 Feb 2;18(1):25. doi: 10.1186/s12886-018-0687-4. BMC Ophthalmol. 2018. PMID: 29394920 Free PMC article.
-
High-Flow Extracranial-Intracranial Bypass for Giant Cavernous Carotid Aneurysm.J Craniofac Surg. 2018 Jun;29(4):1042-1046. doi: 10.1097/SCS.0000000000004422. J Craniofac Surg. 2018. PMID: 29554063
-
Post-traumatic Cavernous Carotid Pseudoaneurysm with Delayed Epistaxis.Cureus. 2018 Jul 19;10(7):e3002. doi: 10.7759/cureus.3002. Cureus. 2018. PMID: 30250764 Free PMC article.
-
Surgical treatment of large and giant cavernous carotid aneurysms.Asian J Neurosurg. 2017 Jul-Sep;12(3):382-388. doi: 10.4103/1793-5482.180930. Asian J Neurosurg. 2017. PMID: 28761512 Free PMC article. Review.
-
Bilateral cavernous carotid aneurysms treated by two-stage extracranial-intracranial bypass followed by parent artery occlusion: case report and literature review.Acta Neurochir (Wien). 2017 Sep;159(9):1693-1698. doi: 10.1007/s00701-017-3101-8. Epub 2017 Feb 8. Acta Neurochir (Wien). 2017. PMID: 28181086 Review.
Cited by
-
Atypical Symptomatic Bilateral Spontaneous Cavernous Carotid Aneurysm with Systemic Vessel Wall Pathology in Young Female: A Rare Case Report.Asian J Neurosurg. 2019 Nov 25;14(4):1245-1248. doi: 10.4103/ajns.AJNS_210_19. eCollection 2019 Oct-Dec. Asian J Neurosurg. 2019. PMID: 31903372 Free PMC article.
-
Spontaneous thrombosis and calcification of giant cavernous carotid artery aneurysm: A rare case and management insights.Surg Neurol Int. 2024 Mar 22;15:98. doi: 10.25259/SNI_805_2023. eCollection 2024. Surg Neurol Int. 2024. PMID: 38628510 Free PMC article.
-
Benign Natural Progression of Small Cavernous Carotid Aneurysms Suggests Limited Clinical Utility of Serial Longitudinal Follow-up.Neurosurgery. 2024 Dec 1;95(6):1441-1449. doi: 10.1227/neu.0000000000003033. Epub 2024 Jun 20. Neurosurgery. 2024. PMID: 38899866 Free PMC article.
References
-
- Ambekar S, Madhugiri V, Sharma M, Cuellar H, Nanda A. Evolution of management strategies for cavernous carotid aneurysms: A review. World Neurosurg. 2014;82:1077–85. - PubMed
-
- Welch BG, Batjer HH. Cavernous carotid aneurysms: You can but should you? World Neurosurg. 2014;82:996–7. - PubMed
-
- Hardy WG, Thomas LM, Webster JE, Gurdjian ES. Carotid ligation for intracranial aneurysm; a follow-up study of 54 patients. J Neurosurg. 1958;15:281–9. - PubMed
-
- Kasliwal MK, Suri A, Sai Kiran NA, Sharma BS. Spontaneous thrombosis of giant cavernous internal carotid artery aneurysm in a neonate. Case report and review of the literature. Pediatr Neurosurg. 2008;44:329–32. - PubMed
-
- Glaiberman CB, Towbin RB, Boal DK. Giant mycotic aneurysm of the internal carotid artery in a child: Endovascular treatment. Pediatr Radiol. 2003;33:211–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources