Large Bowel Obstruction in the Emergency Department: Imaging Spectrum of Common and Uncommon Causes
- PMID: 28480123
- PMCID: PMC5404618
- DOI: 10.4103/jcis.JCIS_6_17
Large Bowel Obstruction in the Emergency Department: Imaging Spectrum of Common and Uncommon Causes
Abstract
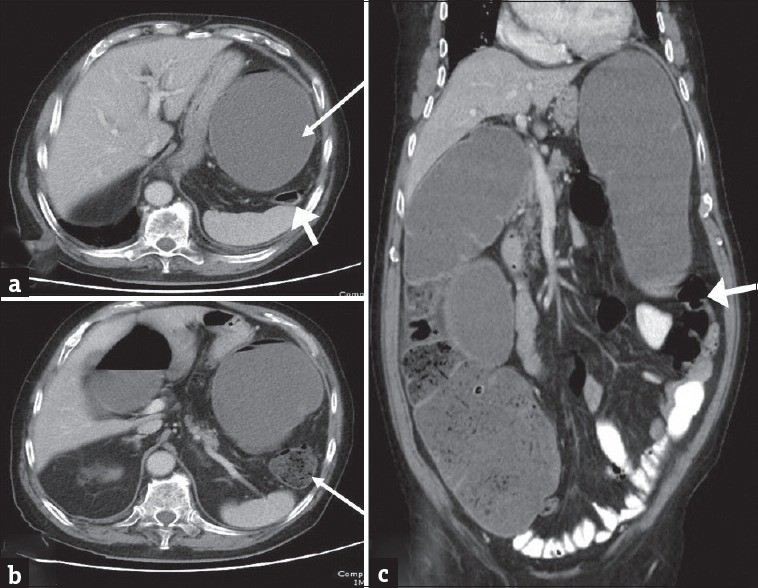
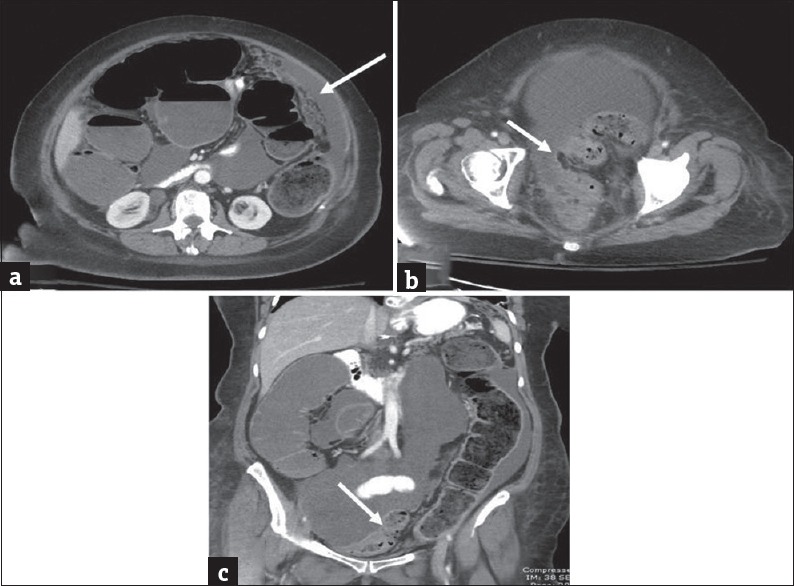
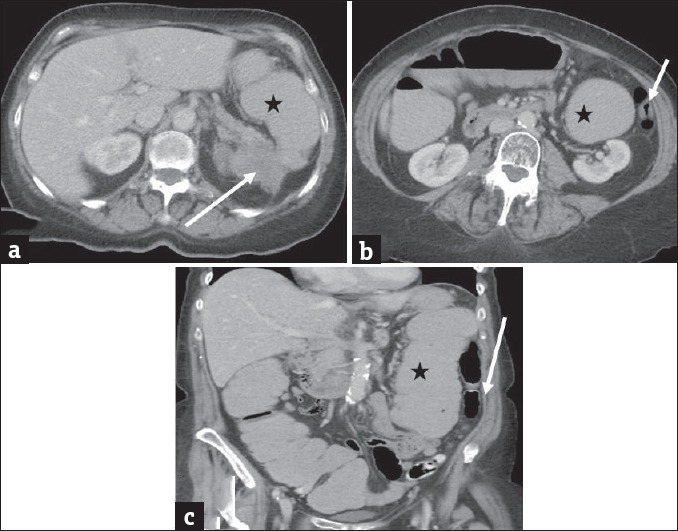
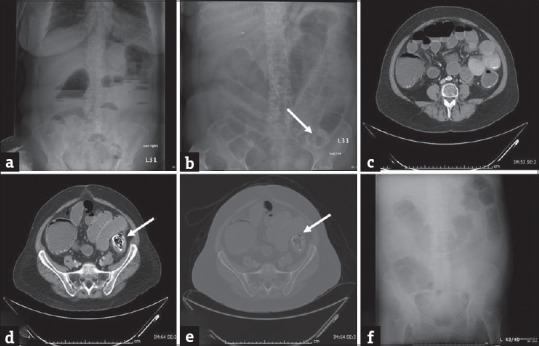
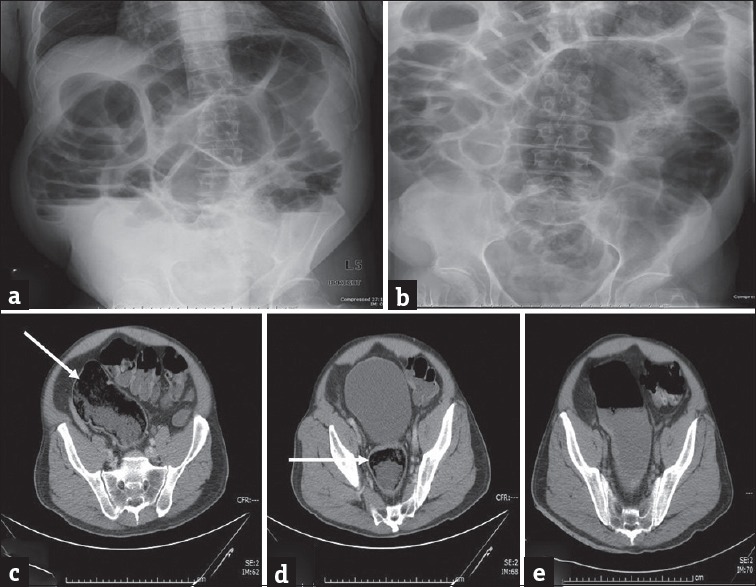
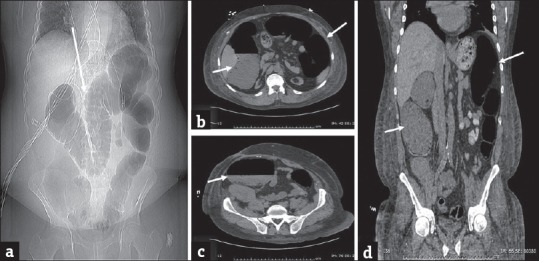
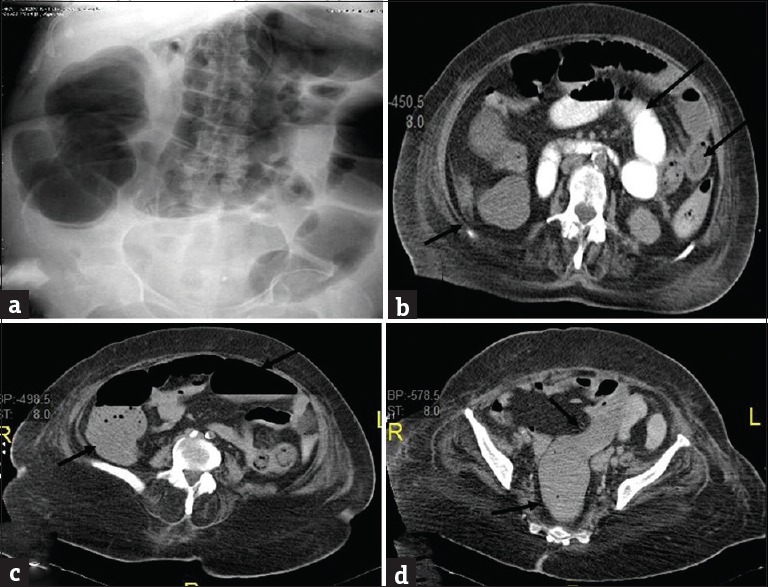
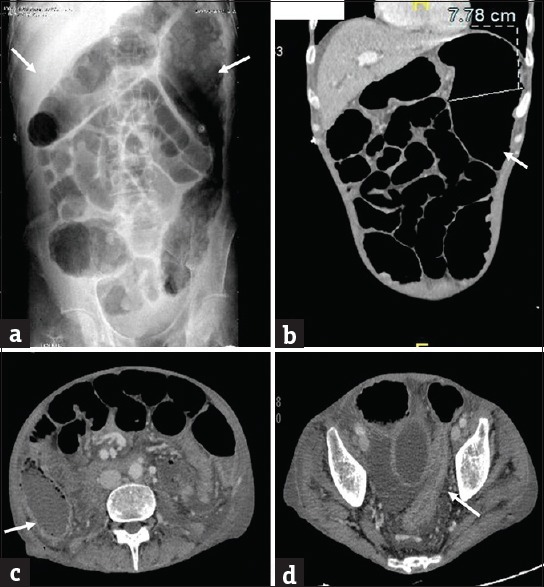
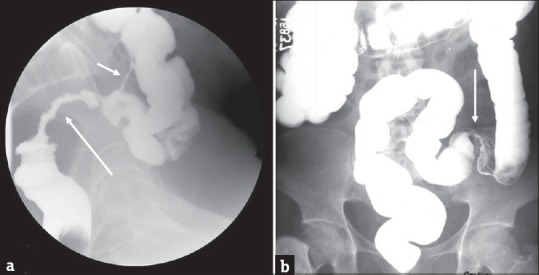
Although large bowel obstruction (LBO) is less common than small bowel obstruction, it is associated with high morbidity and mortality due to delayed diagnosis and/or treatment. Plain radiographs are sufficient to diagnose LBO in a majority of patients. However, further evaluation with multidetector computed tomography (MDCT) has become the standard of care to identify the site, severity, and etiology of obstruction. In this comprehensive review, we illustrate the various causes of LBO emphasizing the role of MDCT in the initial diagnosis and detection of complications along with the tips to differentiate from disease which can mimic LBO.
Keywords: Diverticulitis; large bowel obstruction; multidetector computed tomography; neoplastic; pseudo-obstruction; volvulus.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Taourel P, Kessler N, Lesnik A, Pujol J, Morcos L, Bruel JM. Helical CT of large bowel obstruction. Abdom Imaging. 2003;28:267–75. - PubMed
-
- Yeo HL, Lee SW. Colorectal emergencies: Review and controversies in the management of large bowel obstruction. J Gastrointest Surg. 2013;17:2007–12. - PubMed
-
- Gore RM, Levine MS, editors. Textbook of Gastrointestinal Radiology. 3rd ed. Philadelphia, PA: Saunders, Elsevier; 2008.
-
- Horton KM, Corl FM, Fishman EK. CT evaluation of the colon: Inflammatory disease. Radiographics. 2000;20:399–418. - PubMed
-
- Frager D, Rovno HD, Baer JW, Bashist B, Friedman M. Prospective evaluation of colonic obstruction with computed tomography. Abdom Imaging. 1998;23:141–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources