

Cost Effectiveness and Cost Containment in the Era of Interferon-Free Therapies to Treat Hepatitis C Virus Genotype 1
- PMID: 28480259
- PMCID: PMC5414108
- DOI: 10.1093/ofid/ofw266
Cost Effectiveness and Cost Containment in the Era of Interferon-Free Therapies to Treat Hepatitis C Virus Genotype 1
Abstract
Background: Interferon-free regimens to treat hepatitis C virus (HCV) genotype 1 are effective but costly. At this time, payers in the United States use strategies to control costs including (1) limiting treatment to those with advanced disease and (2) negotiating price discounts in exchange for exclusivity.
Methods: We used Monte Carlo simulation to investigate budgetary impact and cost effectiveness of these treatment policies and to identify strategies that balance access with cost control. Outcomes included nondiscounted 5-year payer cost per 10000 HCV-infected patients and incremental cost-effectiveness ratios.
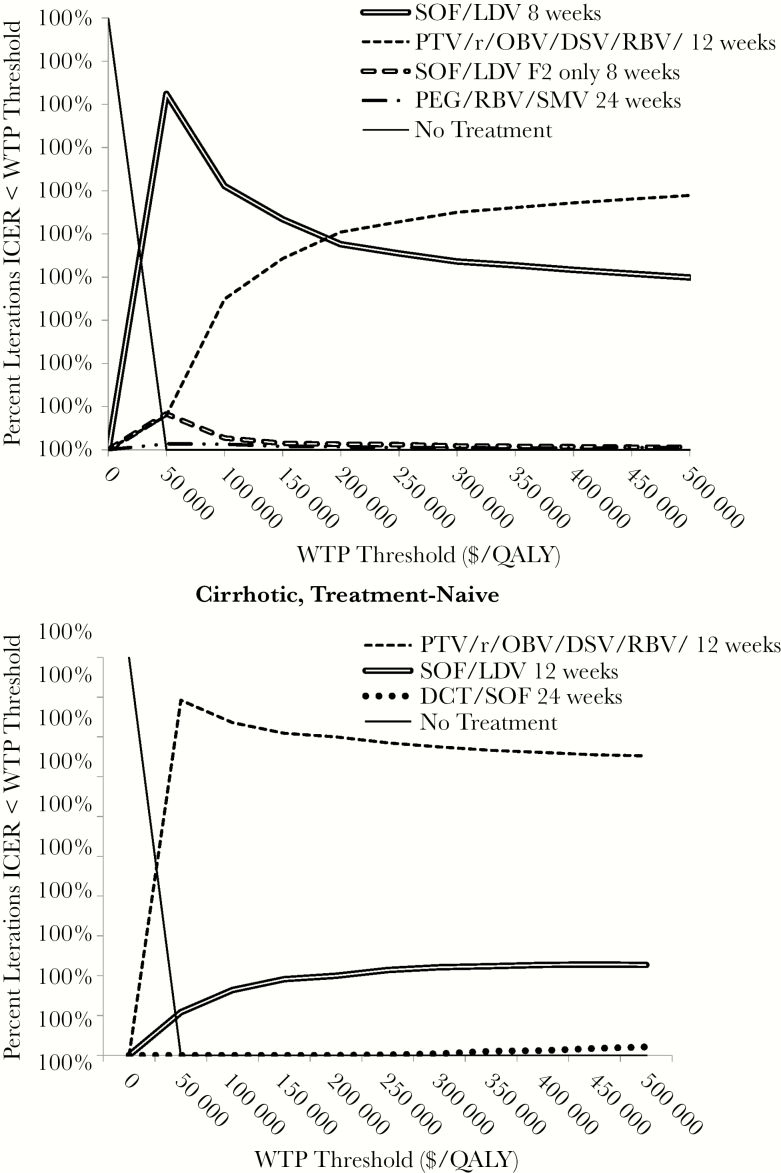
Results: We found that the budgetary impact of HCV treatment is high, with 5-year undiscounted costs of $1.0 billion to 2.3 billion per 10000 HCV-infected patients depending on regimen choices. Among noncirrhotic patients, using the least costly interferon-free regimen leads to the lowest payer costs with negligible difference in clinical outcomes, even when the lower cost regimen is less convenient and/or effective. Among cirrhotic patients, more effective but costly regimens remain cost effective. Controlling costs by restricting treatment to those with fibrosis stage 2 or greater disease was cost ineffective for any patient type compared with treating all patients.
Conclusions: Treatment strategies using interferon-free therapies to treat all HCV-infected persons are cost effective, but short-term cost is high. Among noncirrhotic patients, using the least costly interferon-free regimen, even if it is not single tablet or once daily, is the cost-control strategy that results in best outcomes. Restricting treatment to patients with more advanced disease often results in worse outcomes than treating all patients, and it is not preferred.
Keywords: HCV; budget impact; treatment restriction.
© The Author 2016. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Micromedex 2.0. Drug Topics Red Book Online. Avalable at: http://www.micromedexsolutions.com Accessed 22 December 2015
-
- Najafzadeh M, Andersson K, Shrank WH, et al. Cost-effectiveness of novel regimens for the treatment of hepatitis C virus. Ann Intern Med 2015; 162:407–19. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
