

Body Temperature after EMS Transport: Association with Traumatic Brain Injury Outcomes
- PMID: 28481163
- PMCID: PMC5638643
- DOI: 10.1080/10903127.2017.1308609
Body Temperature after EMS Transport: Association with Traumatic Brain Injury Outcomes
Abstract
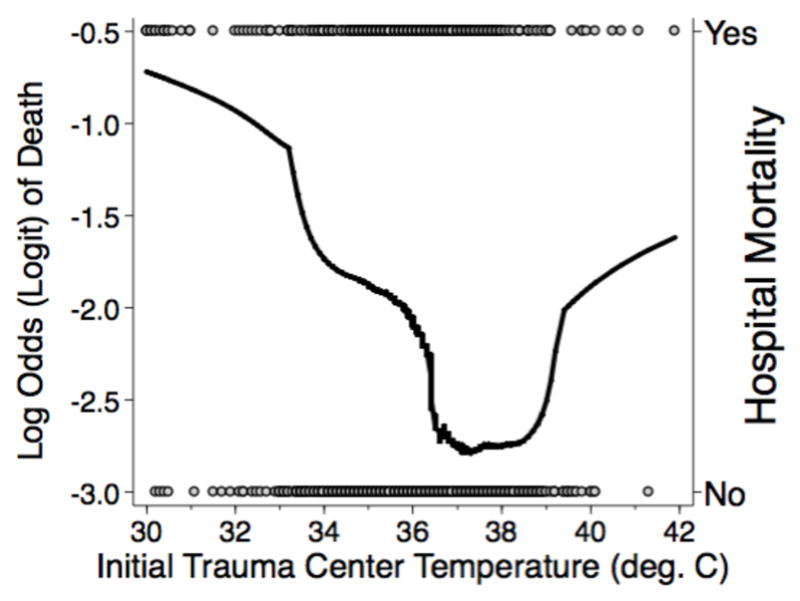
Introduction: Low body temperatures following prehospital transport are associated with poor outcomes in patients with traumatic brain injury (TBI). However, a minimal amount is known about potential associations across a range of temperatures obtained immediately after prehospital transport. Furthermore, a minimal amount is known about the influence of body temperature on non-mortality outcomes. The purpose of this study was to assess the correlation between temperatures obtained immediately following prehospital transport and TBI outcomes across the entire range of temperatures.
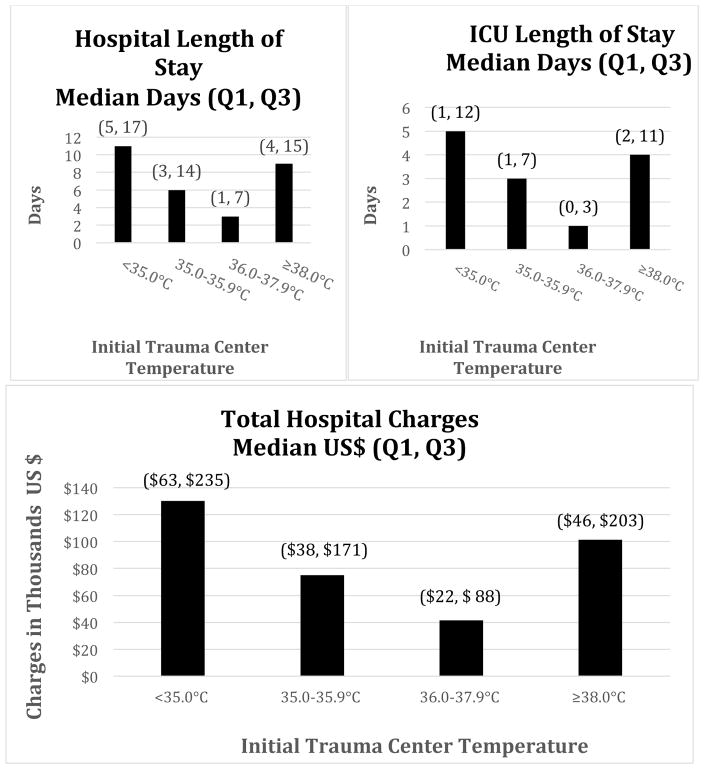
Methods: This retrospective observational study included all moderate/severe TBI cases (CDC Barell Matrix Type 1) in the pre-implementation cohort of the Excellence in Prehospital Injury Care (EPIC) TBI Study (NIH/NINDS: 1R01NS071049). Cases were compared across four cohorts of initial trauma center temperature (ITCT): <35.0°C [Very Low Temperature (VLT)]; 35.0-35.9°C [Low Temperature (LT)]; 36.0-37.9°C [Normal Temperature (NT)]; and ≥38.0°C [Elevated Temperature (ET)]. Multivariable analysis was performed adjusting for injury severity score, age, sex, race, ethnicity, blunt/penetrating trauma, and payment source. Adjusted odds ratios (aORs) with 95% confidence intervals (CI) for mortality were calculated. To evaluate non-mortality outcomes, deaths were excluded and the adjusted median increase in hospital length of stay (LOS), ICU LOS and total hospital charges were calculated for each ITCT group and compared to the NT group.
Results: 22,925 cases were identified and cases with interfacility transfer (7361, 32%), no EMS transport (1213, 5%), missing ITCT (2083, 9%), or missing demographic data (391, 2%) were excluded. Within this study cohort the aORs for death (compared to the NT group) were 2.41 (CI: 1.83-3.17) for VLT, 1.62 (CI: 1.37-1.93) for LT, and 1.86 (CI: 1.52-3.00) for ET. Similarly, trauma center (TC) LOS, ICU LOS, and total TC charges increased in all temperature groups when compared to NT.
Conclusion: In this large, statewide study of major TBI, both ETs and LTs immediately following prehospital transport were independently associated with higher mortality and with increased TC LOS, ICU LOS, and total TC charges. Further study is needed to identify the causes of abnormal body temperature during the prehospital interval and if in-field measures to prevent temperature variations might improve outcomes.
Keywords: cost; hyperthermia; hypothermia; mortality; traumatic brain injury.
Figures
Similar articles
-
Association of Statewide Implementation of the Prehospital Traumatic Brain Injury Treatment Guidelines With Patient Survival Following Traumatic Brain Injury: The Excellence in Prehospital Injury Care (EPIC) Study.JAMA Surg. 2019 Jul 1;154(7):e191152. doi: 10.1001/jamasurg.2019.1152. Epub 2019 Jul 17. JAMA Surg. 2019. PMID: 31066879 Free PMC article.
-
Statin discontinuation and mortality in an older adult population with traumatic brain injury: A four-year, multi-centre, observational cohort study.Injury. 2017 May;48(5):1040-1046. doi: 10.1016/j.injury.2016.11.027. Epub 2016 Nov 25. Injury. 2017. PMID: 27914661
-
Hospital volume-outcome relationship in severe traumatic brain injury: stratified analysis by level of trauma center.J Neurosurg. 2020 Mar 13;134(3):1303-1315. doi: 10.3171/2020.1.JNS192115. Print 2021 Mar 1. J Neurosurg. 2020. PMID: 32168482
-
Effect of Physician-Staffed Emergency Medical Services (P-EMS) on the Outcome of Patients with Severe Traumatic Brain Injury: A Review of the Literature.Prehosp Emerg Care. 2019 Sep-Oct;23(5):730-739. doi: 10.1080/10903127.2019.1575498. Epub 2019 Mar 15. Prehosp Emerg Care. 2019. PMID: 30693835 Review.
-
Environmental Hyperthermia in Prehospital Patients with Major Traumatic Brain Injury.J Emerg Med. 2015 Sep;49(3):375-81. doi: 10.1016/j.jemermed.2015.01.038. Epub 2015 Jul 7. J Emerg Med. 2015. PMID: 26159904 Review.
Cited by
-
Prediction of Mortality in Geriatric Traumatic Brain Injury Patients Using Machine Learning Algorithms.Brain Sci. 2023 Jan 3;13(1):94. doi: 10.3390/brainsci13010094. Brain Sci. 2023. PMID: 36672075 Free PMC article.
-
Rapid prediction of secondary neurologic decline after traumatic brain injury: a data analytic approach.Sci Rep. 2023 Jan 9;13(1):403. doi: 10.1038/s41598-022-26318-4. Sci Rep. 2023. PMID: 36624110 Free PMC article.
-
Impact of fever on the outcome non-anoxic acute brain injury patients: a systematic review and meta-analysis.Crit Care. 2024 Nov 13;28(1):367. doi: 10.1186/s13054-024-05132-6. Crit Care. 2024. PMID: 39538310 Free PMC article.
-
Performance of Modified Early Warning Score (MEWS) for Predicting In-Hospital Mortality in Traumatic Brain Injury Patients.J Clin Med. 2021 Apr 28;10(9):1915. doi: 10.3390/jcm10091915. J Clin Med. 2021. PMID: 33925023 Free PMC article.
References
-
- Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21:375–8. - PubMed
-
- Faul M National Center for Injury Prevention and Control (U.S.) Traumatic brain injury in the United States emergency department visits, hospitalizations, and deaths, 2002–2006. 2010
-
- Finkelstein ECP, Miller TR. The incidence and economic burden of injuries in the United States. New York: Oxford University Press; 2006.
-
- Corrigan JD, Selassie AW, Orman JA. The epidemiology of traumatic brain injury. J Head Trauma Rehabil. 2010;25:72–80. - PubMed
-
- Thurman DJ, Alverson C, Dunn KA, Guerrero J, Sniezek JE. Traumatic brain injury in the United States: A public health perspective. J Head Trauma Rehabil. 1999;14:602–15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials