

The Effect of Isomaltulose Together with Green Tea on Glycemic Response and Antioxidant Capacity: A Single-Blind, Crossover Study in Healthy Subjects
- PMID: 28481230
- PMCID: PMC5452194
- DOI: 10.3390/nu9050464
The Effect of Isomaltulose Together with Green Tea on Glycemic Response and Antioxidant Capacity: A Single-Blind, Crossover Study in Healthy Subjects
Abstract
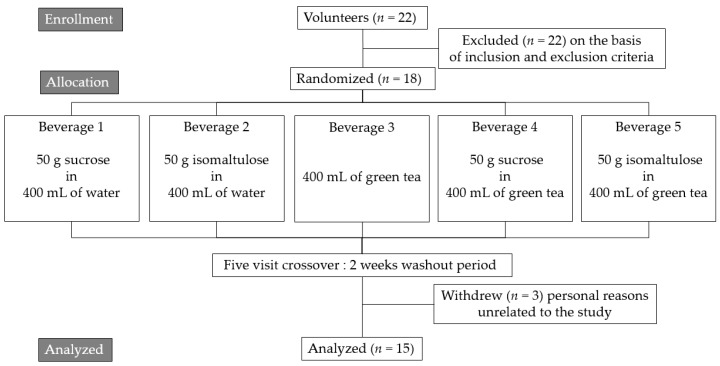
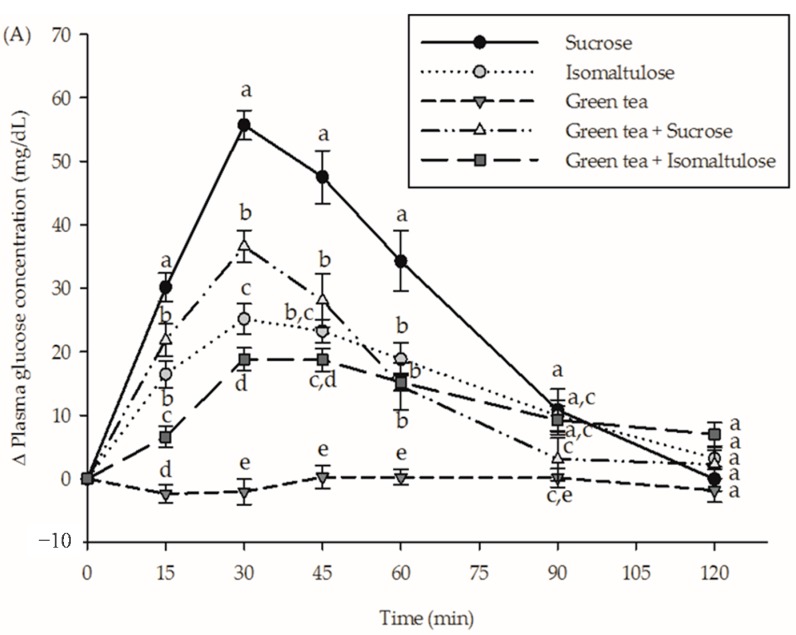
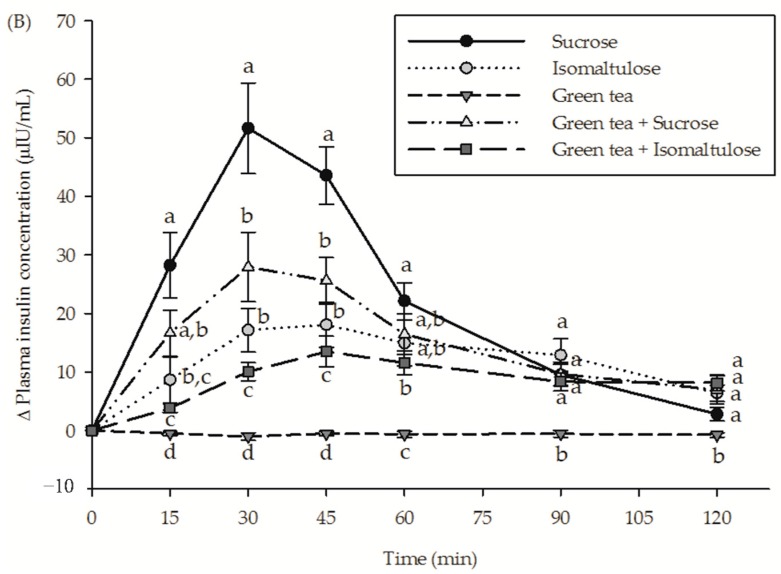
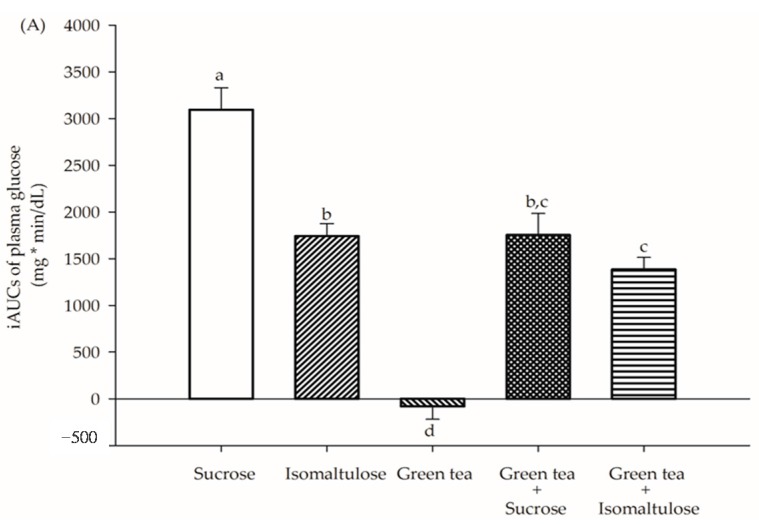
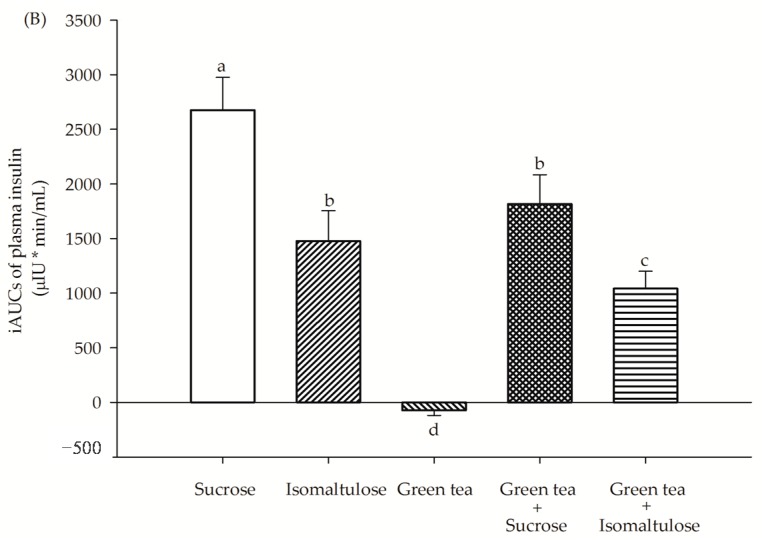
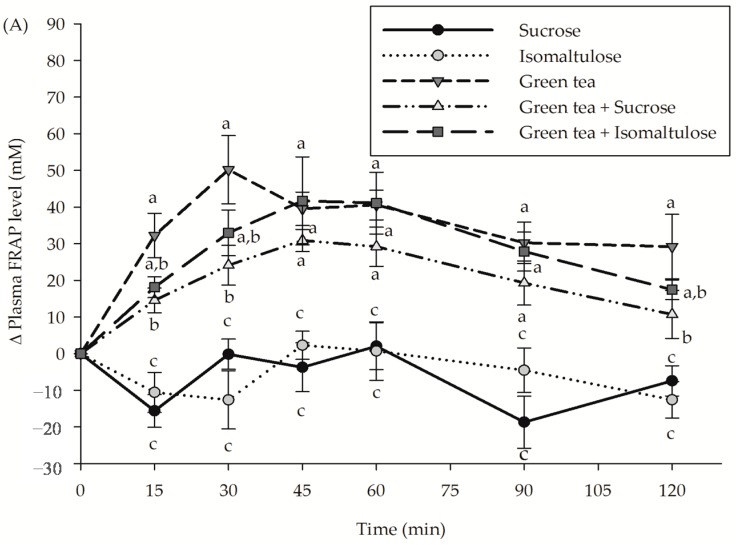
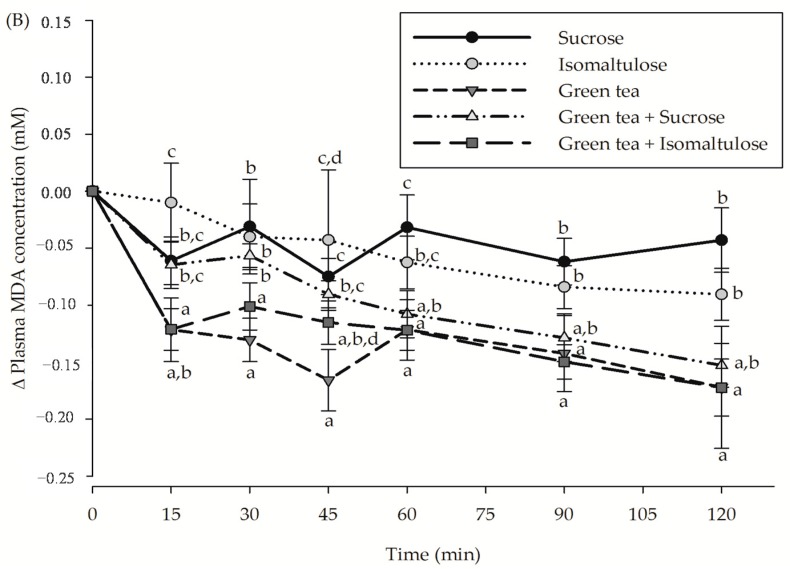
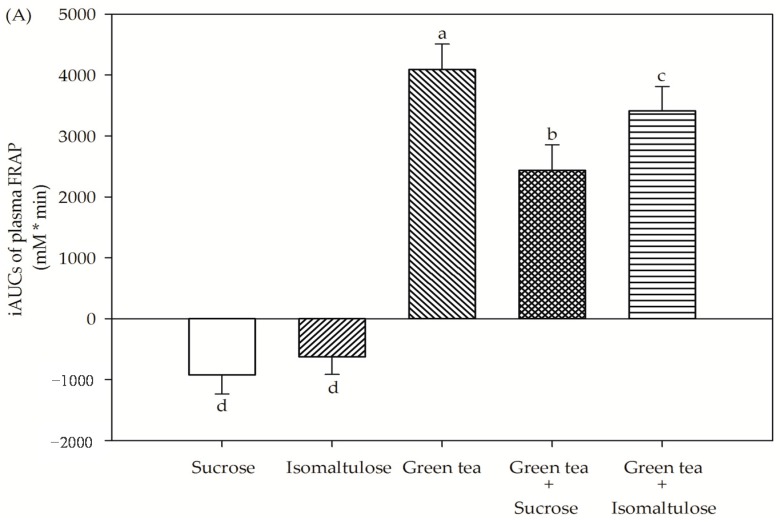
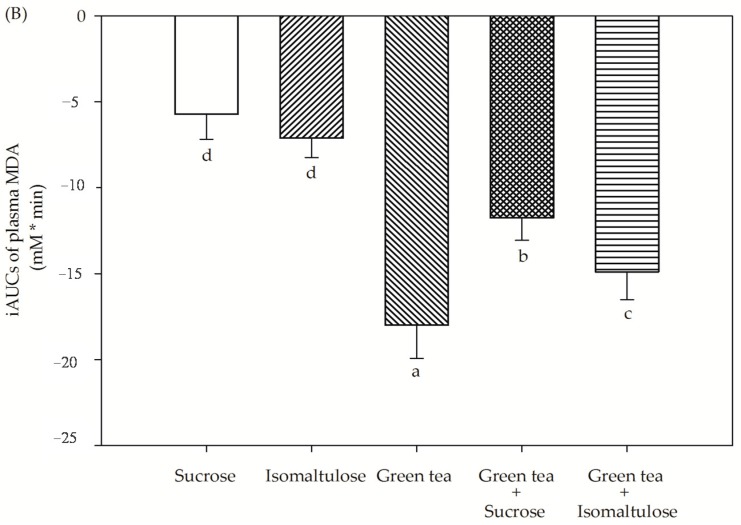
Isomaltulose, a naturally-occurring isomer of sucrose, is commonly used as an alternative sweetener in foods and beverages. The goal of this study was to determine the effect of isomaltulose together with green tea on postprandial plasma glucose and insulin concentration, as well as antioxidant capacity in healthy subjects. In a randomized, single-blind, crossover study, 15 healthy subjects (eight women and seven men; ages 23.5 ± 0.7 years; with body mass index of 22.6 ± 0.4 kg/m²) consumed five beverages: (1) 50 g sucrose in 400 mL water; (2) 50 g isomaltulose in 400 mL of water; (3) 400 mL of green tea; (4) 50 g sucrose in 400 mL of green tea; and (5) 50 g isomaltulose in 400 mL of green tea. Incremental area under postprandial plasma glucose, insulin, ferric reducing ability of plasma (FRAP) and malondialdehyde (MDA) concentration were determined during 120 min of administration. Following the consumption of isomaltulose, the incremental 2-h area under the curve (AUC0-2 h) indicated a higher reduction of postprandial glucose (43.4%) and insulin concentration (42.0%) than the consumption of sucrose. The addition of green tea to isomaltulose produced a greater suppression of postprandial plasma glucose (20.9%) and insulin concentration (37.7%). In accordance with antioxidant capacity, consumption of sucrose (40.0%) and isomaltulose (28.7%) caused the reduction of green tea-induced postprandial increases in FRAP. A reduction in postprandial MDA after drinking green tea was attenuated when consumed with sucrose (34.7%) and isomaltulose (17.2%). In conclusion, green tea could enhance the reduction of postprandial glucose and insulin concentration when consumed with isomaltulose. In comparison with sucrose, isomaltulose demonstrated less alteration of plasma antioxidant capacity after being consumed with green tea.
Keywords: antioxidant capacity; glycemic response; green tea; isomaltulose; sucrose.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Raben A., Vasilaras T.H., Moller A.C., Astrup A. Sucrose compared with artificial sweeteners: Different effects on ad libitum food intake and body weight after 10 week of supplementation in overweight subjects. Am. J. Clin. Nutr. 2002;76:721–729. - PubMed
-
- Moraes P.C.B.T., Bolini H.M.A. Different sweeteners in beverages prepared with instant and roasted ground coffee: Ideal and equivalent sweetness. J. Sens. Stud. 2010;25:215–225. doi: 10.1111/j.1745-459X.2010.00275. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
