

Contribution of the PDL to Osteotomy Repair and Implant Osseointegration
- PMID: 28481696
- PMCID: PMC5502960
- DOI: 10.1177/0022034517707513
Contribution of the PDL to Osteotomy Repair and Implant Osseointegration
Abstract
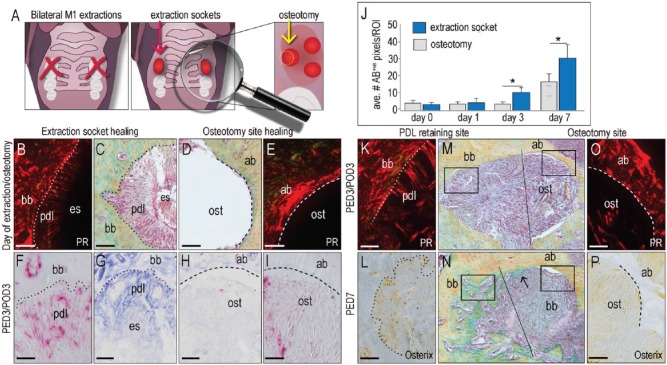
Our objective was to clarify the fate of the periodontal ligament (PDL) retained in the socket after tooth extraction, then determine if this tissue contributed to the osseointegration of "immediate" implants placed in these fresh extraction sockets. Mice underwent maxillary first molar extraction, the residual PDL was removed by an osteotomy, and titanium implants were placed. The osteotomy was created in such a way that the palatal surface was devoid of PDL remnants while the buccal, mesial, and distal surfaces retained PDL fibers. At multiple time points after surgery, tissues were analyzed using a battery of molecular, cellular, and histomorphometrical assays. We found that PDL remnants mineralized and directly contributed to new bone formation in the extraction site. Compared with regions of an extraction site where the PDL was removed by osteotomy, regions that retained PDL fibers had produced significantly more new bone. Around immediate implants, the retained PDL remnants directly contributed to new bone formation and osseointegration. Thus, we conclude that PDL remnants are inherently osteogenic, and if the tissue is healthy, it is reasonable to conclude that curetting out an extraction socket prior to immediate implant placement should be avoided. This recommendation aligns with contemporary trends toward minimally invasive surgical manipulations of the extraction socket prior to immediate implant placement.
Keywords: bone; extraction socket; histology; immediate implant; periostin; regeneration.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Figures



References
-
- Ahn JJ, Shin HI. 2008. Bone tissue formation in extraction sockets from sites with advanced periodontal disease: a histomorphometric study in humans. Int J Oral Maxillofac Implants. 23(6):1133–1138. - PubMed
-
- Albrektsson T, Branemark PI, Hansson HA, Lindstrom J. 1981. Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop Scand. 52(2):155–170. - PubMed
-
- Araújo MG, Lindhe J. 2005. Dimensional ridge alterations following tooth extraction: an experimental study in the dog. J Clin Periodontol. 32(2):212–218. - PubMed
-
- Barzilay I, Graser GN, Iranpour B, Proskin HM. 1996. Immediate implantation of pure titanium implants into extraction sockets of Macaca fascicularis. Part I: Clinical and radiographic assessment. Int J Oral Maxillofac Implants. 11(3):299–310. - PubMed
-
- Becker W. 2006. Immediate implant placement: treatment planning and surgical steps for successful outcomes. Br Dent J. 201(4):199–205. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
