

Elective cesarean section for women living with HIV: a systematic review of risks and benefits
- PMID: 28481770
- PMCID: PMC5491238
- DOI: 10.1097/QAD.0000000000001535
Elective cesarean section for women living with HIV: a systematic review of risks and benefits
Abstract
Objective and design: To inform WHO guidelines, we conducted a systematic review and meta-analysis to assess maternal and perinatal outcomes comparing cesarean section (c-section) before labor and rupture of membranes [elective c-section (ECS)] with other modes of delivery for women living with HIV.
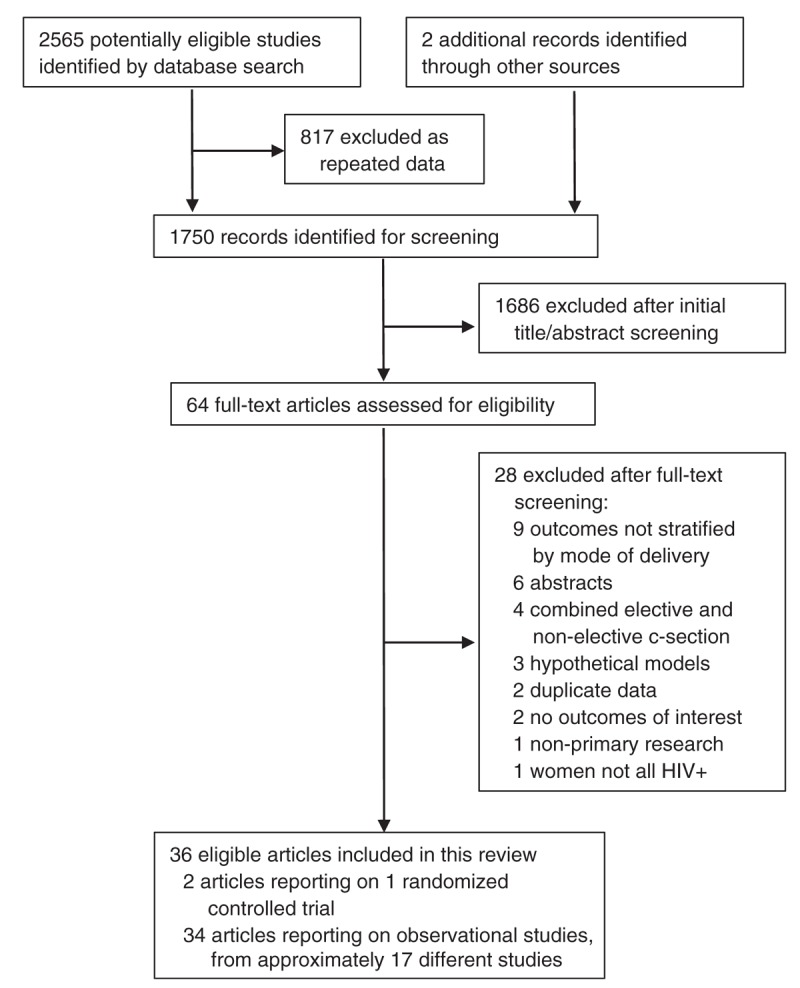
Methods: We searched PubMed, CINAHL, Embase, CENTRAL, and previous reviews to identify published trials and observational studies through October 2015. Results were synthesized using random-effects meta-analysis, stratifying for combination antiretroviral therapy (cART), CD4/viral load (VL), delivery at term, and low-income/middle-income countries.
Results: From 2567 citations identified, 36 articles met inclusion criteria. The single randomized trial, published in 1999, reported minimal maternal morbidity and significantly fewer infant HIV infections with ECS [odds ratio (OR) 0.2, 95% confidence interval (CI) 0.0-0.5]. Across observational studies, ECS was associated with increased maternal morbidity compared with vaginal delivery (OR 3.12, 95% CI 2.21-4.41). ECS was also associated with decreased infant HIV infection overall (OR 0.43, 95% CI 0.30-0.63) and in low-income/middle-income countries (OR 0.27, 95% CI 0.16-0.45), but not among women on cART (OR 0.82, 95% CI 0.47-1.43) or with CD4 cell count more than 200/VL less than 400/term delivery (OR 0.59, 95% CI 0.21-1.63). Infant morbidity moderately increased with ECS.
Conclusion: Although ECS may reduce infant HIV infection, this effect was not statistically significant in the context of cART and viral suppression. As ECS poses other risks, routine ECS for all women living with HIV may not be appropriate. Risks and benefits will differ across settings, depending on underlying risks of ECS complications and vertical transmission during delivery. Understanding individual client risks and benefits and respecting women's autonomy remain important.
Figures
References
-
- The International Perinatal HIV Group. The mode of delivery and the risk of vertical transmission of human immunodeficiency virus type 1: a meta-analysis of 15 prospective cohort studies. N Engl J Med 1999; 340:977–987. - PubMed
-
- World Health Organization. Guideline on when to start antiretroviral therapy and on preexposure prophylaxis for HIV. Geneva, Switzerland: WHO; September 2015. Available from: http://apps.who.int/iris/bitstream/10665/186275/1/9789241509565_eng.pdf?... [Accessed 24 April 2017]
-
- World Health Organization. WHO statement on caesarean section rates 2015. Geneva, Switzerland: WHO; 2015. Available from: http://apps.who.int/iris/bitstream/10665/161442/1/WHO_RHR_15.02_eng.pdf?... [Accessed 24 April 2017]
-
- Read JS, Newell MK. Efficacy and safety of cesarean delivery for prevention of mother-to-child transmission of HIV-1. Cochrane Database Syst Rev 2005; 4: CD005479. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
