

Risk of Nontargeted Infectious Disease Hospitalizations Among US Children Following Inactivated and Live Vaccines, 2005-2014
- PMID: 28481979
- PMCID: PMC5879781
- DOI: 10.1093/cid/cix442
Risk of Nontargeted Infectious Disease Hospitalizations Among US Children Following Inactivated and Live Vaccines, 2005-2014
Abstract
Background: Recent studies have shown that some vaccines have beneficial effects that cannot be explained solely by the prevention of their respective targeted disease(s).
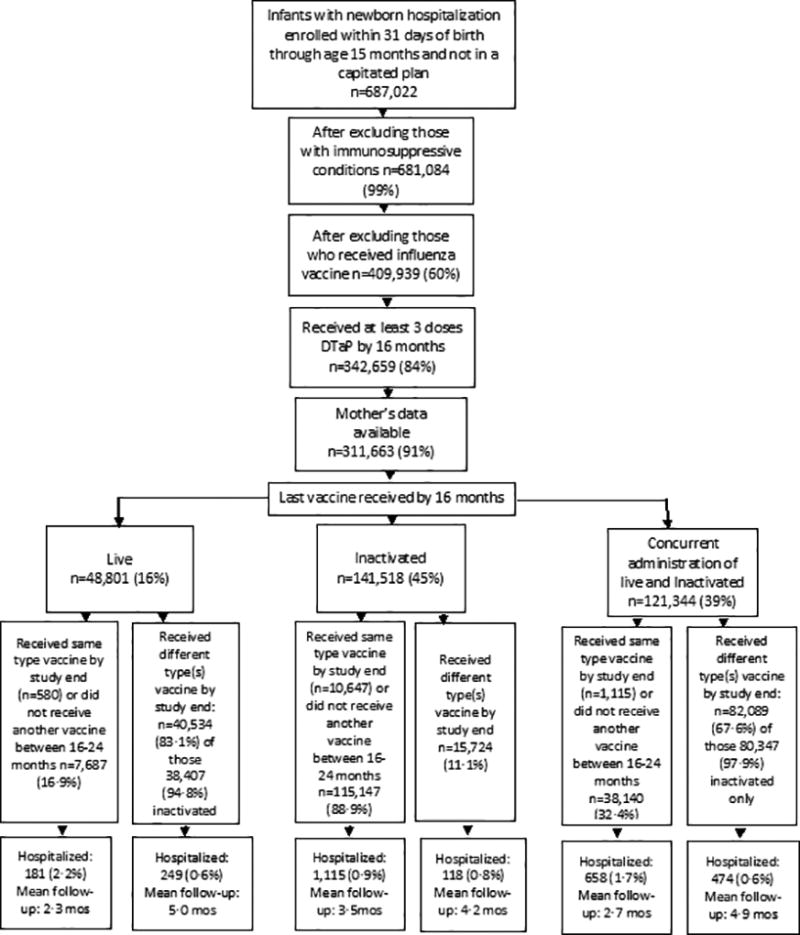
Methods: We used the MarketScan US Commercial Claims Databases for 2005 to 2014 to assess the risk of hospital admission for nontargeted infectious (NTI) diseases in children aged 16 through 24 months according to the last vaccine type (live and/or inactivated). We included children continuously enrolled within a month of birth through 15 months who received at least 3 doses of diphtheria-tetanus-acellular pertussis vaccine by the end of 15 months of age. We used Cox regression to estimate hazard ratios (HRs), stratifying by birthdate to control for age, year, and seasonality and adjusting for sex, chronic diseases, prior hospitalizations, number of outpatient visits, region of residence, urban/rural area of domicile, prematurity, low birth weight, and mother's age.
Results: 311663 children were included. In adjusted analyses, risk of hospitalization for NTI from ages 16 through 24 months was reduced for those who received live vaccine alone compared with inactivated alone or concurrent live and inactivated vaccines (HR, 0.50; 95% confidence interval [CI], 0.43, 0.57 and HR, 0.78; 95% CI, 0.67, 0.91, respectively) and for those who received live and inactivated vaccines concurrently compared with inactivated-only (HR, 0.64; 95% CI, 0.58, 0.70).
Conclusions: We found lower risk of NTI disease hospitalizations from age 16 through 24 months among children whose last vaccine received was live compared with inactivated vaccine, as well as concurrent receipt compared with inactivated vaccine.
Keywords: heterologous immunity; infant immunization; marketscan; nontargeted infectious diseases; safety of vaccination schedule.
Published by Oxford University Press for the Infectious Diseases Society of America 2017. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Conflict of interest statement
All authors declare no competing interests.
Comment in
-
Growth Parameters, Effect Measure Modification and the Association Between Vaccination and Early Childhood Hospitalization With Non-targeted Infections.Clin Infect Dis. 2018 Jan 6;66(2):318-319. doi: 10.1093/cid/cix838. Clin Infect Dis. 2018. PMID: 29325082 No abstract available.
-
Reply to Burgner, et al.Clin Infect Dis. 2018 Jan 6;66(2):319. doi: 10.1093/cid/cix839. Clin Infect Dis. 2018. PMID: 29325083 Free PMC article. No abstract available.
References
-
- Biering-Sorensen S, Aaby P, Napirna BM, et al. Small randomized trial among low-birth-weight children receiving bacillus Calmette-Guerin vaccination at first health center contact. The Pediatric infectious disease journal. 2012;31:306–308. - PubMed
-
- Sorup S, Benn CS, Poulsen A, Krause TG, Aaby P, Ravn H. Live vaccine against measles, mumps, and rubella and the risk of hospital admissions for nontargeted infections. Jama. 2014;311:826–835. - PubMed
-
- Truven Health Analytics. Marketscan Research. 2016 http://marketscan.truvenhealth.com/marketscanportal.
-
- Hansen L, Chang S. White Paper Health Research Data for the Real World: The MarketScan Databases. 2016 http://truvenhealth.com/portals/0/assets/PH_11238_0612_TEMP_MarketScan_W..., 2016.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
