

Preoperative evaluation of accessory hepatic ducts by drip infusion cholangiography with CT
- PMID: 28482819
- PMCID: PMC5422935
- DOI: 10.1186/s12893-017-0251-9
Preoperative evaluation of accessory hepatic ducts by drip infusion cholangiography with CT
Abstract
Background: This retrospective study aimed to investigate the incidence of each type of accessory hepatic duct by drip infusion cholangiography with CT (DIC-CT).
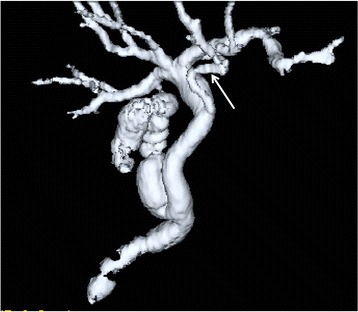
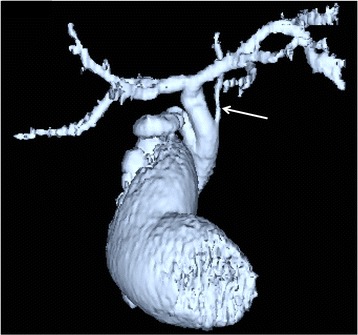
Methods: Five hundred sixty nine patients who underwent preoperative DIC-CT and laparoscopic cholecystectomy were reviewed. Accessory hepatic ducts were classified as follows: type I (accessory hepatic ducts that merged with the common hepatic duct between the confluence of the right and left hepatic ducts and the cystic duct confluence), type II (those that merged with the common hepatic duct at the same site as the cystic duct), type III (those that merged with the common bile duct distal to the cystic duct confluence), type IV (the cystic duct merged with the accessory hepatic duct), and type V (accessory hepatic ducts that merged with the common hepatic or bile duct on the left side).
Results: Accessory hepatic ducts were observed in 50 patients. Type I, II, III, IV, and V accessory hepatic ducts were detected in 32, 3, 1, 11, and 3 patients, respectively. Based on their drainage areas, the accessory hepatic ducts were also classified as follows: a posterior branch in 22 patients, an anterior branch in 9 patients, a combination of posterior and anterior branches in 16 patients, a left-sided branch in 2 patients, and a caudate branch in 1 patient. None of the patients with accessory hepatic ducts suffered bile duct injuries.
Conclusion: There are a number of variants of the accessory hepatic duct. DIC-CT is useful to detect the accessory hepatic duct.
Keywords: Accessory hepatic duct; Bile duct injury; Drip infusion cholangiography with CT; Laparoscopic cholecystectomy.
Figures





References
-
- Ochiai T, Yamazaki S, Ohta K, Takahashi M, Iwai T, Irie T, et al. Is drip infusion cholecystocholangiography (DIC) an acceptable modality at cholecystectomy for cholecystolithiasis, considering the frequency of bile duct maljunction and intraoperative bile duct injury? J Hepato-Biliary-Pancreat Surg. 2004;11:135–139. doi: 10.1007/s00534-003-0873-4. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
