

Disturbed microcirculation in the hands of patients with systemic sclerosis detected by fluorescence optical imaging: a pilot study
- PMID: 28482872
- PMCID: PMC5422953
- DOI: 10.1186/s13075-017-1300-6
Disturbed microcirculation in the hands of patients with systemic sclerosis detected by fluorescence optical imaging: a pilot study
Abstract
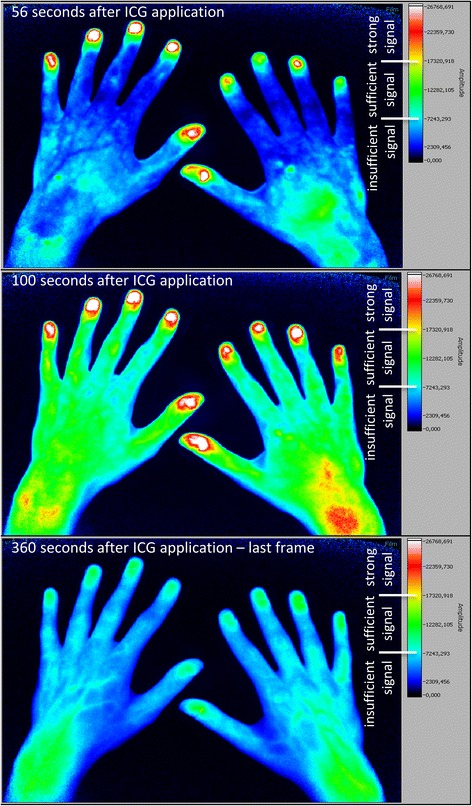
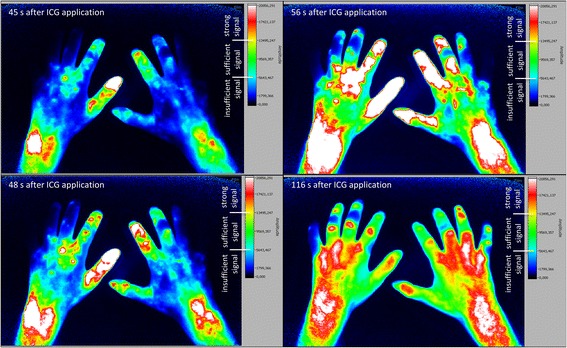
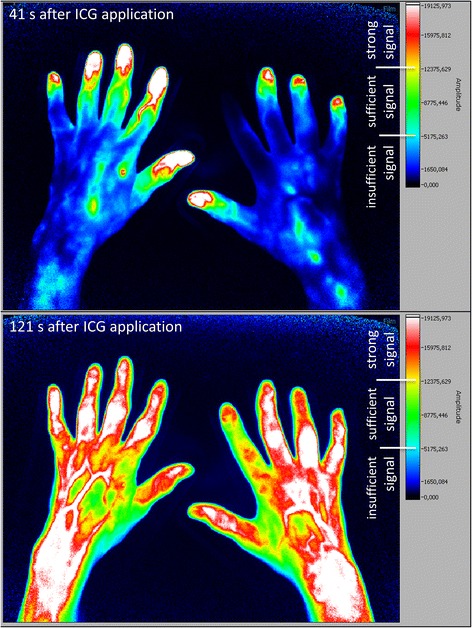
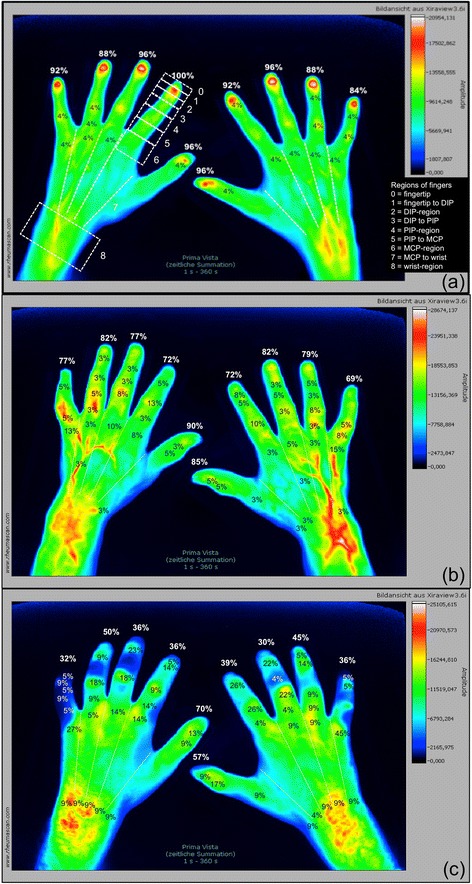
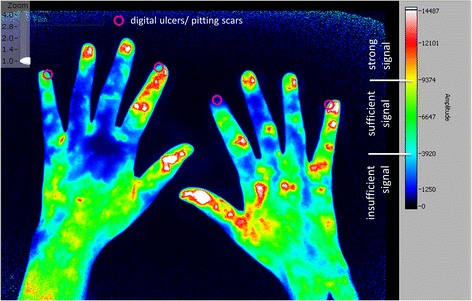
Background: Utilising fluorescence optical imaging (FOI), the distribution of an intravenously applied colouring agent indocyanine green (ICG) can be analysed with the potential to identify malperfusion by little to no tissue enhancement. Systemic sclerosis (SSc) is characterised by the presence of digital ulcers reflecting progressive vasculopathy. The objective was to investigate the potential of FOI in the detection of disturbed microcirculation in the hands and fingers of patients with SSc and to link FOI findings to clinical signs of ischemia such as digital ulcers and pitting scars.
Methods: In this cross-sectional study, 63 patients with SSc and 26 healthy subjects were examined. FOI was performed in all 89 individuals and compared to clinical data and capillaroscopic findings assembled for the SSc cohort.
Results: Healthy subjects showed initial ICG signals in their fingertips in 93.6%, SSc patients in 78.5% (limited SSc) and 43.2% (diffuse SSc). Moreover, in SSc patients, FOI findings were significantly associated with a late capillaroscopic pattern, disseminated SSc features, a diffuse SSc subtype, and the presence of digital ulcers or pitting scars. Intra- and inter-reader reliability for FOI amounted to κ = 0.786 and κ = 0.834, respectively.
Conclusions: FOI is able to detect areas of reduced microcirculation in patients with SSc with high association to capillaroscopic findings. The results pave the way for future FOI investigations into its role in the prediction of complications due to an impaired acral perfusion.
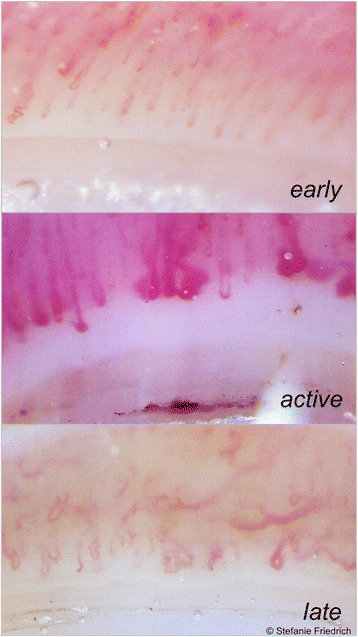
Keywords: Digital ulcers; Disturbed microcirculation; Fluorescence optical imaging; Nailfold capillaroscopy; Raynaud’s phenomenon; Systemic sclerosis.
Figures
References
-
- Glimm AM, Werner SG, Burmester GR, et al. Analysis of distribution and severity of inflammation in patients with osteoarthitis compared to rheumatoid arthritis by ICG-enhanced fluorescence optical imaging and musculoskeletal ultrasound: a pilot study. Ann Rheum Dis. 2016;75(3):566–70. doi:10.1136/annrheumdis-2015-207345. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
