

Severe Delayed Cutaneous and Systemic Reactions to Drugs: A Global Perspective on the Science and Art of Current Practice
- PMID: 28483310
- PMCID: PMC5424615
- DOI: 10.1016/j.jaip.2017.01.025
Severe Delayed Cutaneous and Systemic Reactions to Drugs: A Global Perspective on the Science and Art of Current Practice
Abstract
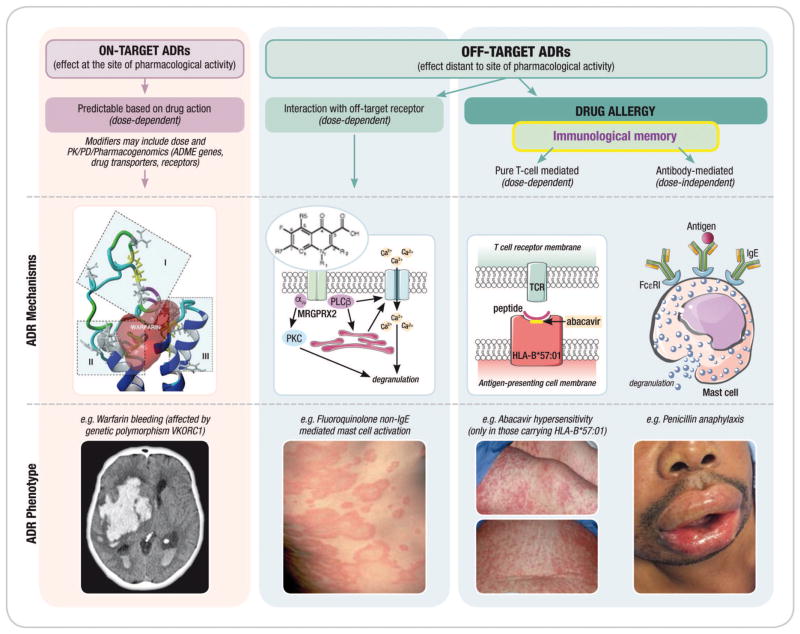
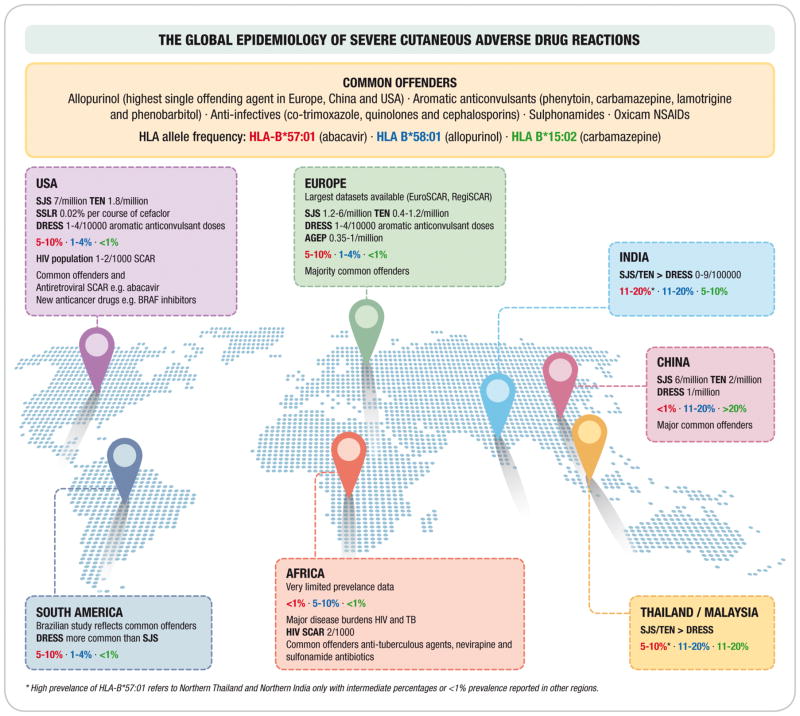
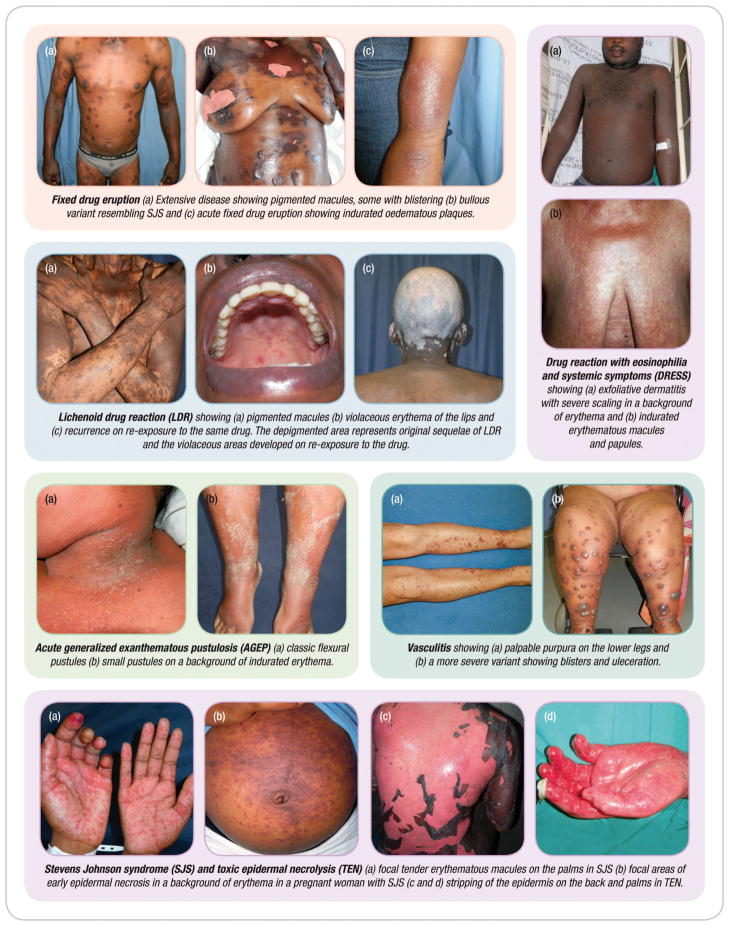
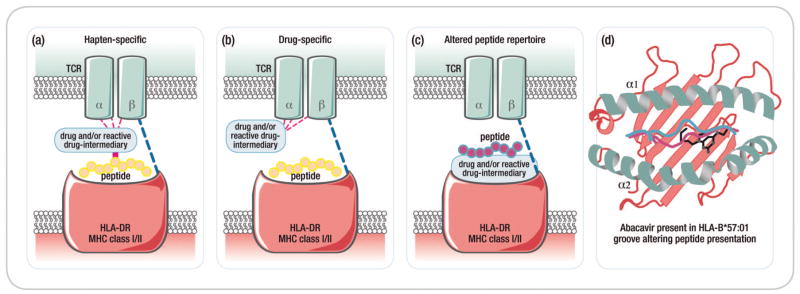
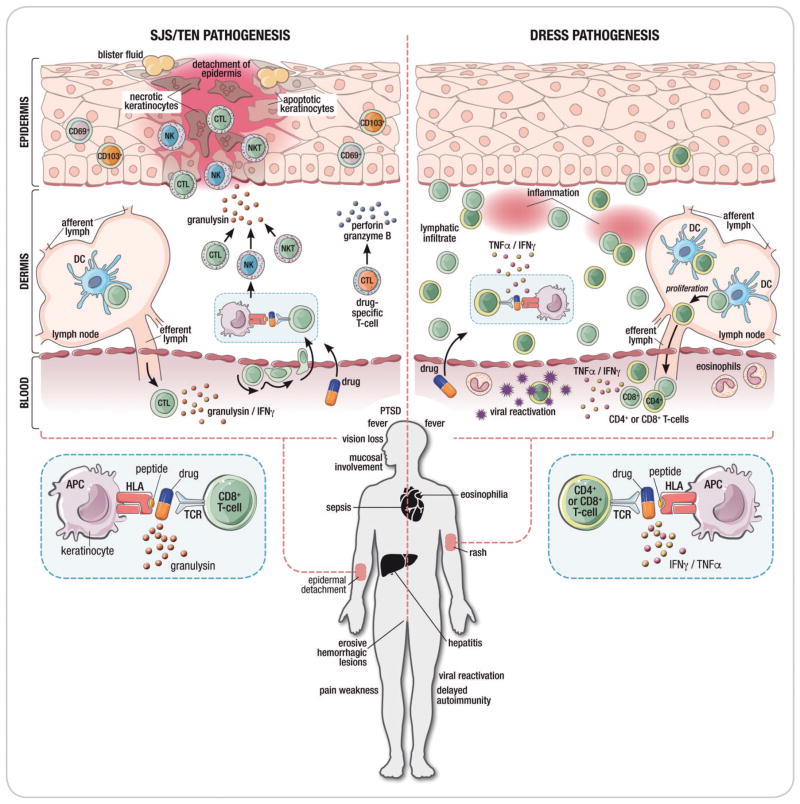
Most immune-mediated adverse drug reactions (IM-ADRs) involve the skin, and many have additional systemic features. Severe cutaneous adverse drug reactions (SCARs) are an uncommon, potentially life-threatening, and challenging subgroup of IM-ADRs with diverse clinical phenotypes, mechanisms, and offending drugs. T-cell-mediated immunopathology is central to these severe delayed reactions, but effector cells and cytokines differ by clinical phenotype. Strong HLA-gene associations have been elucidated for specific drug-SCAR IM-ADRs such as Stevens-Johnson syndrome/toxic epidermal necrolysis, although the mechanisms by which carriage of a specific HLA allele is necessary but not sufficient for the development of many IM-ADRs is still being defined. SCAR management is complicated by substantial short- and long-term morbidity/mortality and the potential need to treat ongoing comorbid disease with related medications. Multidisciplinary specialist teams at experienced units should care for patients. In the setting of SCAR, patient outcomes as well as preventive, diagnostic, treatment, and management approaches are often not generalizable, but rather context specific, driven by population HLA-genetics, the pharmacology and genetic risk factors of the implicated drug, severity of underlying comorbid disease necessitating ongoing treatments, and cost considerations. In this review, we update the basic and clinical science of SCAR diagnosis and management.
Keywords: DRESS; HLA; Immune-mediated adverse drug reactions; SJS/TEN; Severe cutaneous adverse drug reactions; T-cell.
Copyright © 2017 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Kinch MS, Haynesworth A, Kinch SL, Hoyer D. An overview of FDA-approved new molecular entities: 1827–2013. Drug discovery today. 2014;19(8):1033–9. - PubMed
-
- Kongkaew C, Noyce PR, Ashcroft DM. Hospital admissions associated with adverse drug reactions: a systematic review of prospective observational studies. The Annals of pharmacotherapy. 2008;42(7):1017–25. - PubMed
-
- Mockenhaupt M. Epidemiology of cutaneous adverse drug reactions. Chemical immunology and allergy. 2012;97:1–17. - PubMed
-
- Huang HY, Luo XQ, Chan LS, Cao ZH, Sun XF, Xu JH. Cutaneous adverse drug reactions in a hospital-based Chinese population. Clinical and experimental dermatology. 2011;36(2):135–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
