

Glucagon-Like Peptide 1 Receptor Activation Augments Cardiac Output and Improves Cardiac Efficiency in Obese Swine After Myocardial Infarction
- PMID: 28483802
- PMCID: PMC5521862
- DOI: 10.2337/db16-1206
Glucagon-Like Peptide 1 Receptor Activation Augments Cardiac Output and Improves Cardiac Efficiency in Obese Swine After Myocardial Infarction
Abstract
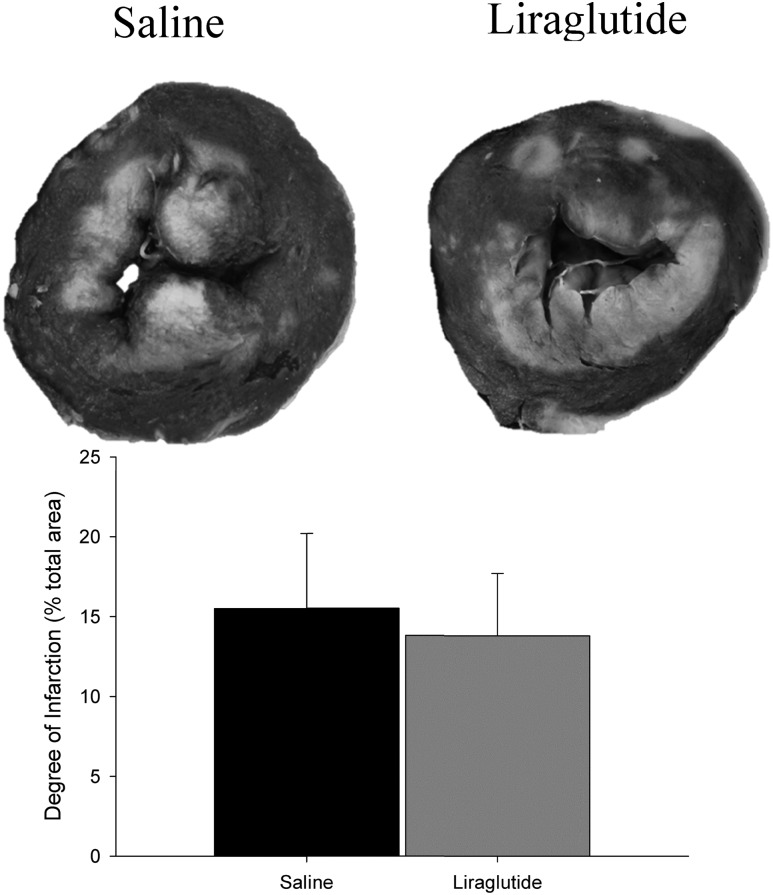
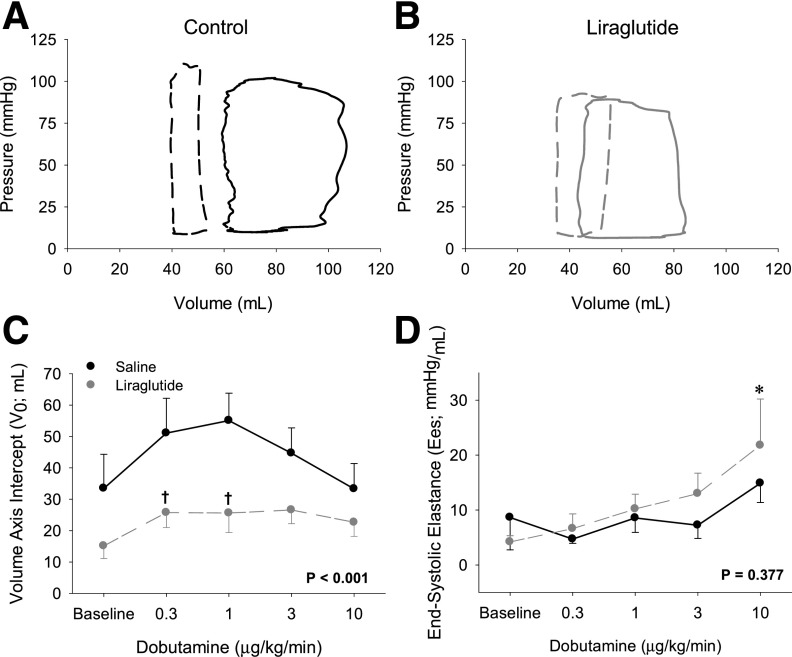
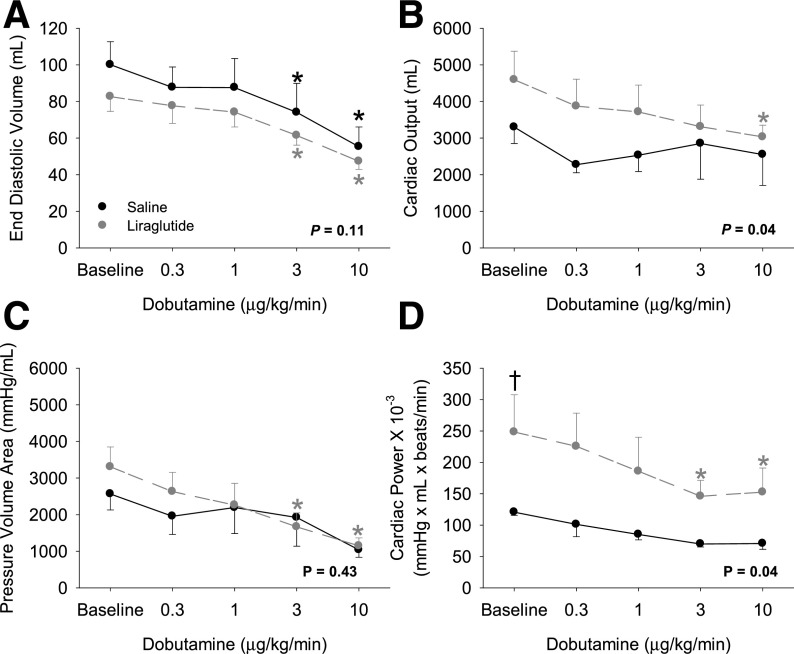
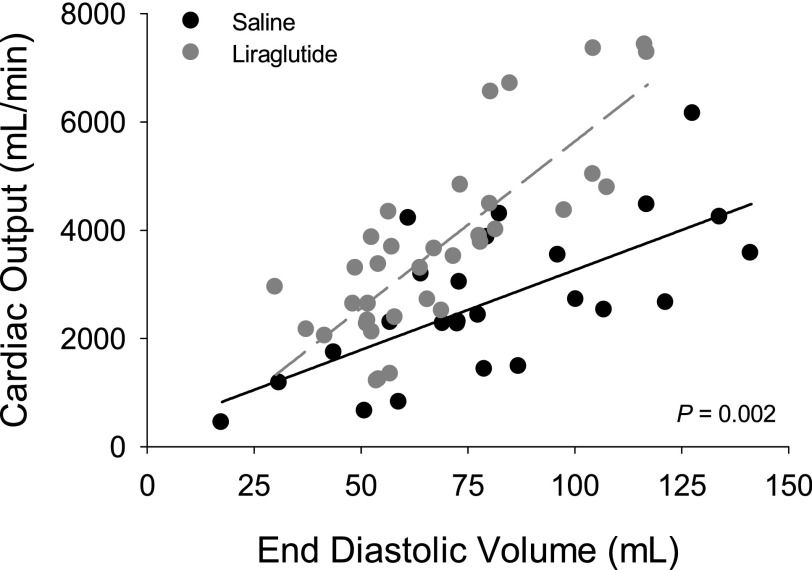
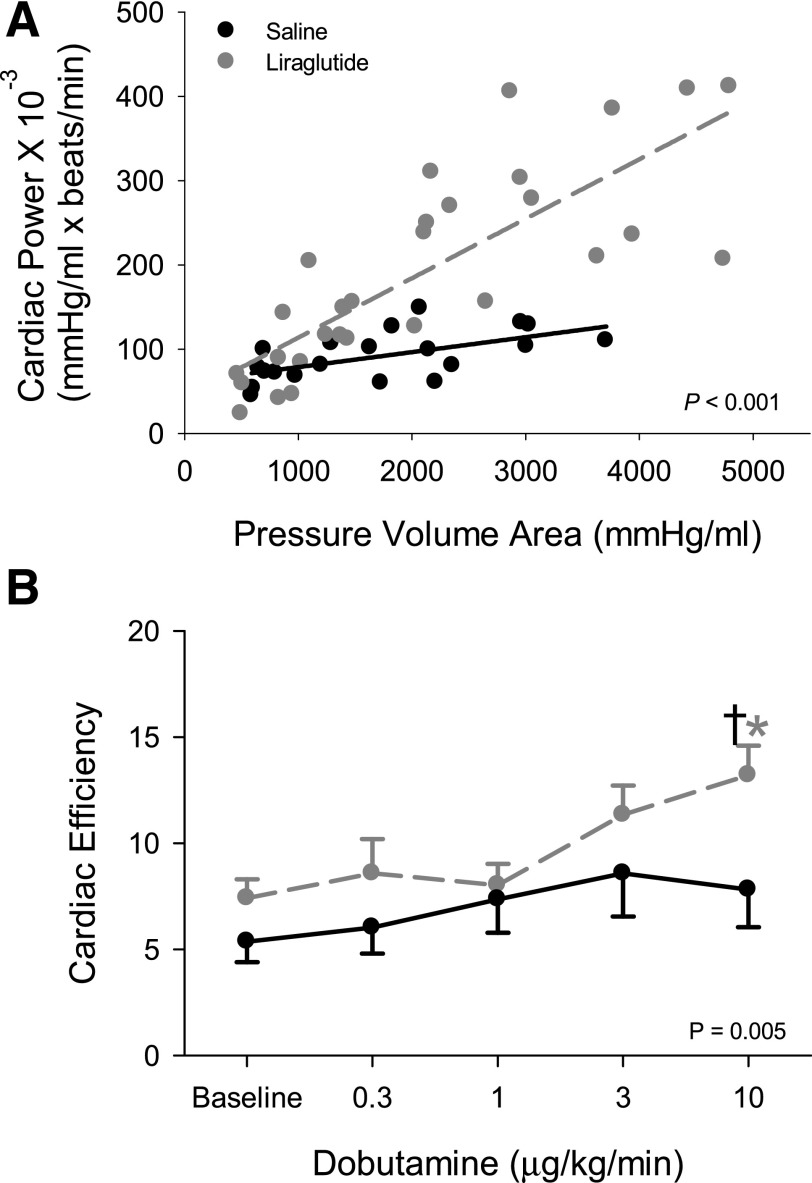
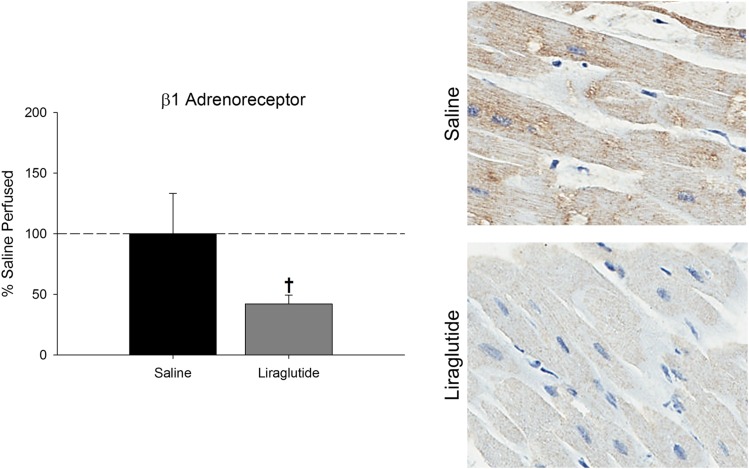
This study tested the hypothesis that glucagon-like peptide 1 (GLP-1) therapies improve cardiac contractile function at rest and in response to adrenergic stimulation in obese swine after myocardial infarction. Obese Ossabaw swine were subjected to gradually developing regional coronary occlusion using an ameroid occluder placed around the left anterior descending coronary artery. Animals received subcutaneous injections of saline or liraglutide (0.005-0.015 mg/kg/day) for 30 days after ameroid placement. Cardiac performance was assessed at rest and in response to sympathomimetic challenge (dobutamine 0.3-10 μg/kg/min) using a left ventricular pressure/volume catheter. Liraglutide increased diastolic relaxation (dP/dt; Tau 1/2; Tau 1/e) during dobutamine stimulation (P < 0.01) despite having no influence on the magnitude of myocardial infarction. The slope of the end-systolic pressure volume relationship (i.e., contractility) increased with dobutamine after liraglutide (P < 0.001) but not saline administration (P = 0.63). Liraglutide enhanced the slope of the relationship between cardiac power and pressure volume area (i.e., cardiac efficiency) with dobutamine (P = 0.017). Hearts from animals treated with liraglutide demonstrated decreased β1-adrenoreceptor expression. These data support that GLP-1 agonism augments cardiac efficiency via attenuation of maladaptive sympathetic signaling in the setting of obesity and myocardial infarction.
© 2017 by the American Diabetes Association.
Figures
Similar articles
-
Lack of effect of prolonged treatment with liraglutide on cardiac remodeling in rats after acute myocardial infarction.Peptides. 2017 Jul;93:1-12. doi: 10.1016/j.peptides.2017.04.009. Epub 2017 Apr 28. Peptides. 2017. PMID: 28460895
-
Vitamin C restores the contractile response to dobutamine and improves myocardial efficiency in patients with heart failure after anterior myocardial infarction.Am Heart J. 2007 Oct;154(4):645.e1-8. doi: 10.1016/j.ahj.2007.07.005. Am Heart J. 2007. PMID: 17892985
-
Effects of liraglutide on left ventricular function in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention.Am Heart J. 2015 Nov;170(5):845-54. doi: 10.1016/j.ahj.2015.07.014. Epub 2015 Jul 26. Am Heart J. 2015. PMID: 26542491 Clinical Trial.
-
Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists in the Treatment of Obese Women with Polycystic Ovary Syndrome.Curr Vasc Pharmacol. 2017;15(3):218-229. doi: 10.2174/1570161114666161221115324. Curr Vasc Pharmacol. 2017. PMID: 28003008 Review.
-
Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists in Cardiac Disorders.Ann Pharmacother. 2016 Dec;50(12):1041-1050. doi: 10.1177/1060028016663218. Epub 2016 Aug 16. Ann Pharmacother. 2016. PMID: 27531946 Review.
Cited by
-
Glucagon-like peptide 1 receptor agonists: cardiovascular benefits and mechanisms of action.Nat Rev Cardiol. 2023 Jul;20(7):463-474. doi: 10.1038/s41569-023-00849-3. Epub 2023 Mar 28. Nat Rev Cardiol. 2023. PMID: 36977782 Review.
-
The pig as an optimal animal model for cardiovascular research.Lab Anim (NY). 2024 Jun;53(6):136-147. doi: 10.1038/s41684-024-01377-4. Epub 2024 May 21. Lab Anim (NY). 2024. PMID: 38773343 Review.
-
Research Progress on the Cardiovascular Protective Effect of Glucagon-Like Peptide-1 Receptor Agonists.J Diabetes Res. 2022 Apr 8;2022:4554996. doi: 10.1155/2022/4554996. eCollection 2022. J Diabetes Res. 2022. PMID: 35434139 Free PMC article. Review.
-
Large Animal Models of Heart Failure: A Translational Bridge to Clinical Success.JACC Basic Transl Sci. 2020 Aug 24;5(8):840-856. doi: 10.1016/j.jacbts.2020.04.011. eCollection 2020 Aug. JACC Basic Transl Sci. 2020. PMID: 32875172 Free PMC article. Review.
-
Chronic high-rate pacing induces heart failure with preserved ejection fraction-like phenotype in Ossabaw swine.Basic Res Cardiol. 2022 Oct 12;117(1):50. doi: 10.1007/s00395-022-00958-z. Basic Res Cardiol. 2022. PMID: 36222894 Free PMC article.
References
-
- Timmers L, Henriques JP, de Kleijn DP, et al. . Exenatide reduces infarct size and improves cardiac function in a porcine model of ischemia and reperfusion injury. J Am Coll Cardiol 2009;53:501–510 - PubMed
-
- Mogensen UM, Andersson C, Fosbøl EL, et al. . Cardiovascular safety of combination therapies with incretin-based drugs and metformin compared with a combination of metformin and sulphonylurea in type 2 diabetes mellitus--a retrospective nationwide study. Diabetes Obes Metab 2014;16:1001–1008 - PubMed
-
- Pfeffer MA, Claggett B, Diaz R, et al. .; ELIXA Investigators . Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med 2015;373:2247–2257 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
