

Treating the dysfunctional placenta
- PMID: 28483805
- PMCID: PMC5516438
- DOI: 10.1530/JOE-17-0185
Treating the dysfunctional placenta
Abstract
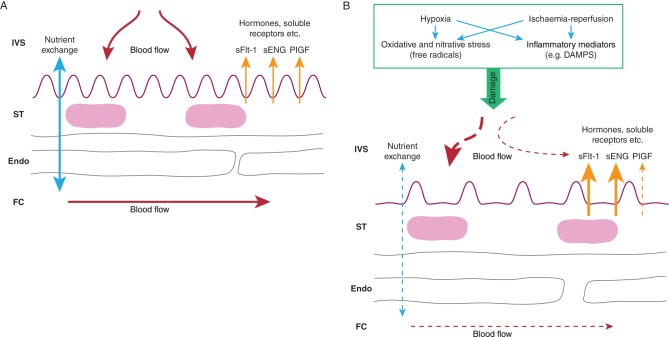
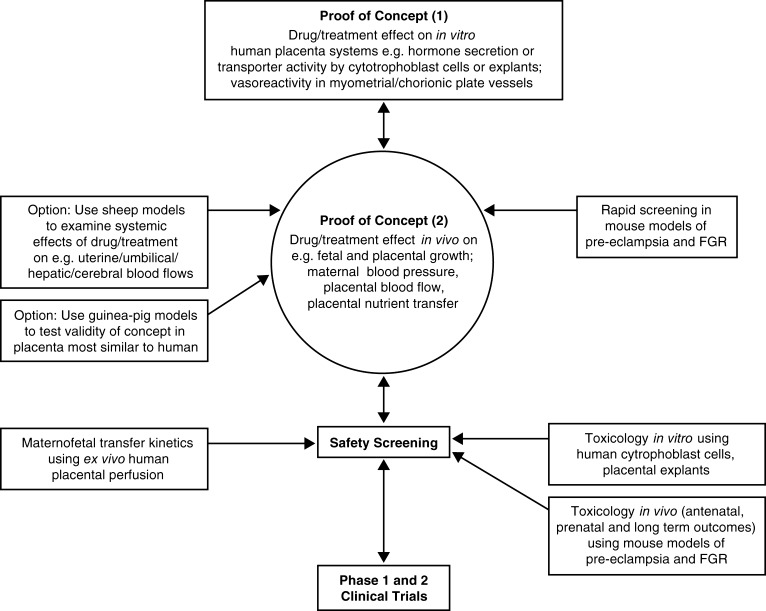
Placental dysfunction underlies major obstetric diseases such as pre-eclampsia and fetal growth restriction (FGR). Whilst there has been a little progress in prophylaxis, there are still no treatments for placental dysfunction in normal obstetric practice. However, a combination of increasingly well-described in vitro systems for studying the human placenta, together with the availability of more appropriate animal models of pre-eclampsia and FGR, has facilitated a recent surge in work aimed at repurposing drugs and therapies, developed for other conditions, as treatments for placental dysfunction. This review: (1) highlights potential candidate drug targets in the placenta - effectors of improved uteroplacental blood flow, anti-oxidants, heme oxygenase induction, inhibition of HIF, induction of cholesterol synthesis pathways, increasing insulin-like growth factor II availability; (2) proposes an experimental pathway for taking a potential drug or treatment for placental dysfunction from concept through to early phase clinical trials, utilizing techniques for studying the human placenta in vitro and small animal models, particularly the mouse, for in vivo studies; (3) describes the data underpinning sildenafil citrate and adenovirus expressing vascular endothelial growth as potential treatments for placental dysfunction and summarizes recent research on other potential treatments. The importance of sharing information from such studies even when no effect is found, or there is an adverse outcome, is highlighted. Finally, the use of adenoviral vectors or nanoparticle carriers coated with homing peptides to selectively target drugs to the placenta is highlighted: such delivery systems could improve efficacy and reduce the side effects of treating the dysfunctional placenta.
Keywords: dysfunction; fetal growth restriction; placenta; pre-eclampsia; treatment.
© 2017 The authors.
Figures
Similar articles
-
The ability of late pregnancy maternal tests to predict adverse pregnancy outcomes associated with placental dysfunction (specifically fetal growth restriction and pre-eclampsia): a protocol for a systematic review and meta-analysis of prognostic accuracy studies.Syst Rev. 2020 Apr 8;9(1):78. doi: 10.1186/s13643-020-01334-5. Syst Rev. 2020. PMID: 32268905 Free PMC article.
-
A placenta clinic approach to the diagnosis and management of fetal growth restriction.Am J Obstet Gynecol. 2018 Feb;218(2S):S803-S817. doi: 10.1016/j.ajog.2017.11.575. Epub 2017 Dec 15. Am J Obstet Gynecol. 2018. PMID: 29254754 Review.
-
Incorporating placental pathology into clinical care and research.Trends Mol Med. 2024 Dec;30(12):1103-1112. doi: 10.1016/j.molmed.2024.08.002. Epub 2024 Sep 18. Trends Mol Med. 2024. PMID: 39299838
-
Placental Drug Delivery to Treat Pre-Eclampsia and Fetal Growth Restriction.Small. 2024 Oct;20(41):e2311165. doi: 10.1002/smll.202311165. Epub 2024 May 15. Small. 2024. PMID: 38745536 Review.
-
Pregnancy outcome and placental findings in pregnancies complicated by fetal growth restriction with and without preeclampsia.Reprod Sci. 2015 Mar;22(3):316-21. doi: 10.1177/1933719114542024. Epub 2014 Jul 6. Reprod Sci. 2015. PMID: 25001023
Cited by
-
PregOMICS-Leveraging systems biology and bioinformatics for drug repurposing in maternal-child health.Am J Reprod Immunol. 2018 Aug;80(2):e12971. doi: 10.1111/aji.12971. Epub 2018 May 4. Am J Reprod Immunol. 2018. PMID: 29726581 Free PMC article.
-
Nanotechnologies in Obstetrics and Cancer during Pregnancy: A Narrative Review.J Pers Med. 2022 Aug 17;12(8):1324. doi: 10.3390/jpm12081324. J Pers Med. 2022. PMID: 36013273 Free PMC article. Review.
-
Unique microRNA Signals in Plasma Exosomes from Pregnancies Complicated by Preeclampsia.Hypertension. 2020 Mar;75(3):762-771. doi: 10.1161/HYPERTENSIONAHA.119.14081. Epub 2020 Jan 27. Hypertension. 2020. PMID: 31983308 Free PMC article.
-
Low-dose aspirin for the prevention of preeclampsia in women with polycystic ovary syndrome: a retrospective cohort study.BMC Pregnancy Childbirth. 2025 Jan 30;25(1):98. doi: 10.1186/s12884-025-07183-1. BMC Pregnancy Childbirth. 2025. PMID: 39885419 Free PMC article.
-
Placenta-Targeted Nanoparticles Loaded with PFKFB3 Overexpression Plasmids Enhance Angiogenesis and Placental Function.Bioengineering (Basel). 2022 Nov 4;9(11):652. doi: 10.3390/bioengineering9110652. Bioengineering (Basel). 2022. PMID: 36354563 Free PMC article.
References
-
- Baschat AB, Galan HL. 2017. Intrauteine growth restriction. In Obstetrics: Normal and Problem Pregnancies, edn 7th, pp 737–7691. Eds Gabbe SG, Niebyl JR, Simpson JL, Landon MB, Galan HL, Jauniaux ERM, Driscoll DA, Berghella V, Grobman WA. Philadelphia, PA, USA: Elsevier.
-
- Brien ME, Duval C, Palacios J, Boufaied I, Hudon-Thibeault AA, Nadeau-Vallée M, Vaillancourt C, Sibley CP, Abrahams VM, Jones RL, et al. 2017. Uric acid crystals induce placental inflammation and alter trophoblast function via an IL-1-dependent pathway: implications for fetal growth restriction. Journal of Immunology 198 443–451. (10.4049/jimmunol.1601179) - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
