

Coronary Plaque Characterization in Psoriasis Reveals High-Risk Features That Improve After Treatment in a Prospective Observational Study
- PMID: 28483812
- PMCID: PMC5534138
- DOI: 10.1161/CIRCULATIONAHA.116.026859
Coronary Plaque Characterization in Psoriasis Reveals High-Risk Features That Improve After Treatment in a Prospective Observational Study
Abstract
Background: Psoriasis, a chronic inflammatory disease associated with an accelerated risk of myocardial infarction, provides an ideal human model to study inflammatory atherogenesis in vivo. We hypothesized that the increased cardiovascular risk observed in psoriasis would be partially attributable to an elevated subclinical coronary artery disease burden composed of noncalcified plaques with high-risk features. However, inadequate efforts have been made to directly measure coronary artery disease in this vulnerable population. As such, we sought to compare total coronary plaque burden and noncalcified coronary plaque burden (NCB) and high-risk plaque (HRP) prevalence between patients with psoriasis (n=105), patients with hyperlipidemia eligible for statin therapy under National Cholesterol Education Program-Adult Treatment Panel III guidelines (n=100) who were ≈10 years older, and healthy volunteers without psoriasis (n=25).
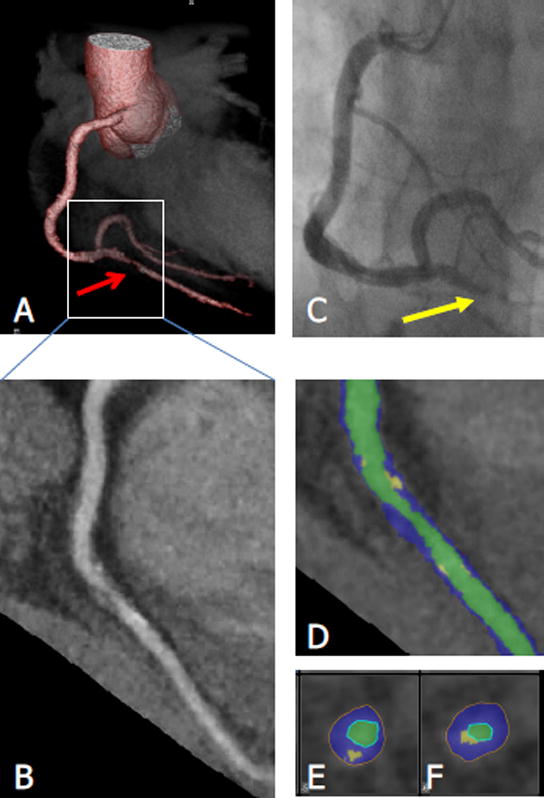
Methods: Patients underwent coronary computed-tomography angiography for total coronary plaque burden and NCB quantification and HRP identification, defined as low attenuation (<30 hounsfield units), positive remodeling (>1.10), and spotty calcification. A consecutive sample of the first 50 patients with psoriasis was scanned again 1 year after therapy.
Results: Despite being younger and at lower traditional risk than patients with hyperlipidemia, patients with psoriasis had increased NCB (mean±SD: 1.18±0.33 versus 1.11±0.32, P=0.02) and similar HRP prevalence (P=0.58). Furthermore, compared to healthy volunteers, patients with psoriasis had increased total coronary plaque burden (1.22±0.31 versus 1.04±0.22, P=0.001), NCB (1.18±0.33 versus 1.03±0.21, P=0.004), and HRP prevalence beyond traditional risk (odds ratio, 6.0; 95% confidence interval, 1.1-31.7; P=0.03). Last, among patients with psoriasis followed for 1 year, improvement in psoriasis severity was associated with improvement in total coronary plaque burden (β=0.45, 0.23-0.67; P<0.001) and NCB (β=0.53, 0.32-0.74; P<0.001) beyond traditional risk factors.
Conclusions: Patients with psoriasis had greater NCB and increased HRP prevalence than healthy volunteers. In addition, patients with psoriasis had elevated NCB and equivalent HRP prevalence as older patients with hyperlipidemia. Last, modulation of target organ inflammation (eg, skin) was associated with an improvement in NCB at 1 year, suggesting that control of remote sites of inflammation may translate into reduced coronary artery disease risk.
Keywords: coronary computed tomography angiography; high-risk plaque; inflammation; noncalcified burden; psoriasis.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
Coronary Plaque Characterization in Psoriasis.Circulation. 2017 Jul 18;136(3):277-280. doi: 10.1161/CIRCULATIONAHA.117.029126. Circulation. 2017. PMID: 28716831 No abstract available.
-
Letter by Jin-shan and Xue-bin Regarding Article, "Coronary Plaque Characterization in Psoriasis Reveals High-Risk Features That Improve After Treatment in a Prospective Observational Study".Circulation. 2018 Mar 6;137(10):1089. doi: 10.1161/CIRCULATIONAHA.117.031391. Circulation. 2018. PMID: 29507001 No abstract available.
-
Letter by Hjuler et al Regarding Article, "Coronary Plaque Characterization in Psoriasis Reveals High-Risk Features That Improve After Treatment in a Prospective Observational Study".Circulation. 2018 Mar 6;137(10):1090-1091. doi: 10.1161/CIRCULATIONAHA.117.029784. Circulation. 2018. PMID: 29507002 No abstract available.
-
Response by Lerman et al to Letters Regarding Article, "Coronary Plaque Characterization in Psoriasis Reveals High-Risk Features That Improve After Treatment in a Prospective Observational Study".Circulation. 2018 Mar 6;137(10):1092-1093. doi: 10.1161/CIRCULATIONAHA.117.031675. Circulation. 2018. PMID: 29507003 Free PMC article. No abstract available.
References
-
- Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA. 2006;296:1735–1741. - PubMed
-
- Hjuler KF, Bottcher M, Vestergaard C, Deleuran M, Raaby L, Botker HE, Iversen L, Kragballe K. Increased Prevalence of Coronary Artery Disease in Severe Psoriasis and Severe Atopic Dermatitis. Am J Med. 2015;128:1325–1334 e2. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
