

JAK/STAT pathway inhibition overcomes IL7-induced glucocorticoid resistance in a subset of human T-cell acute lymphoblastic leukemias
- PMID: 28484265
- PMCID: PMC5729333
- DOI: 10.1038/leu.2017.136
JAK/STAT pathway inhibition overcomes IL7-induced glucocorticoid resistance in a subset of human T-cell acute lymphoblastic leukemias
Abstract
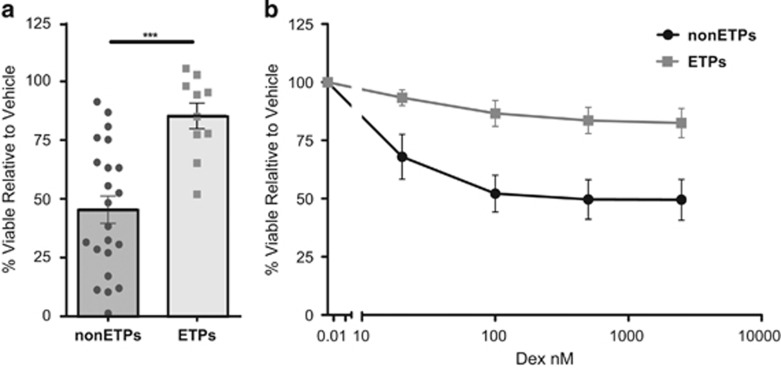
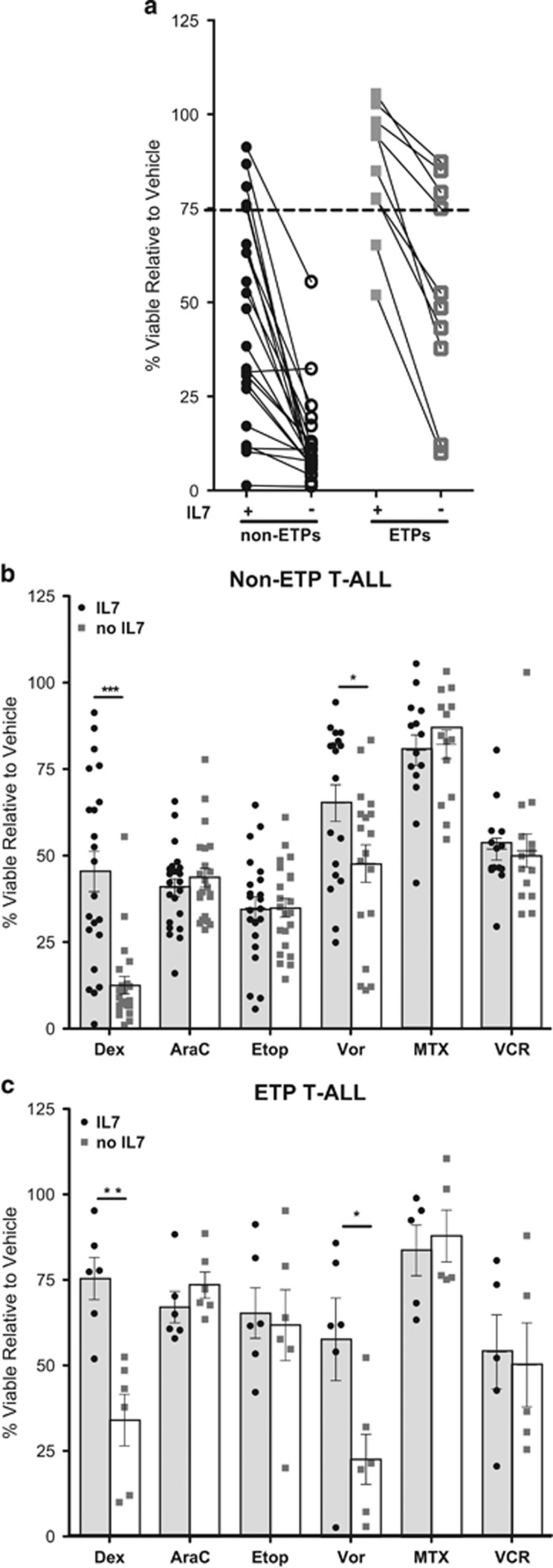
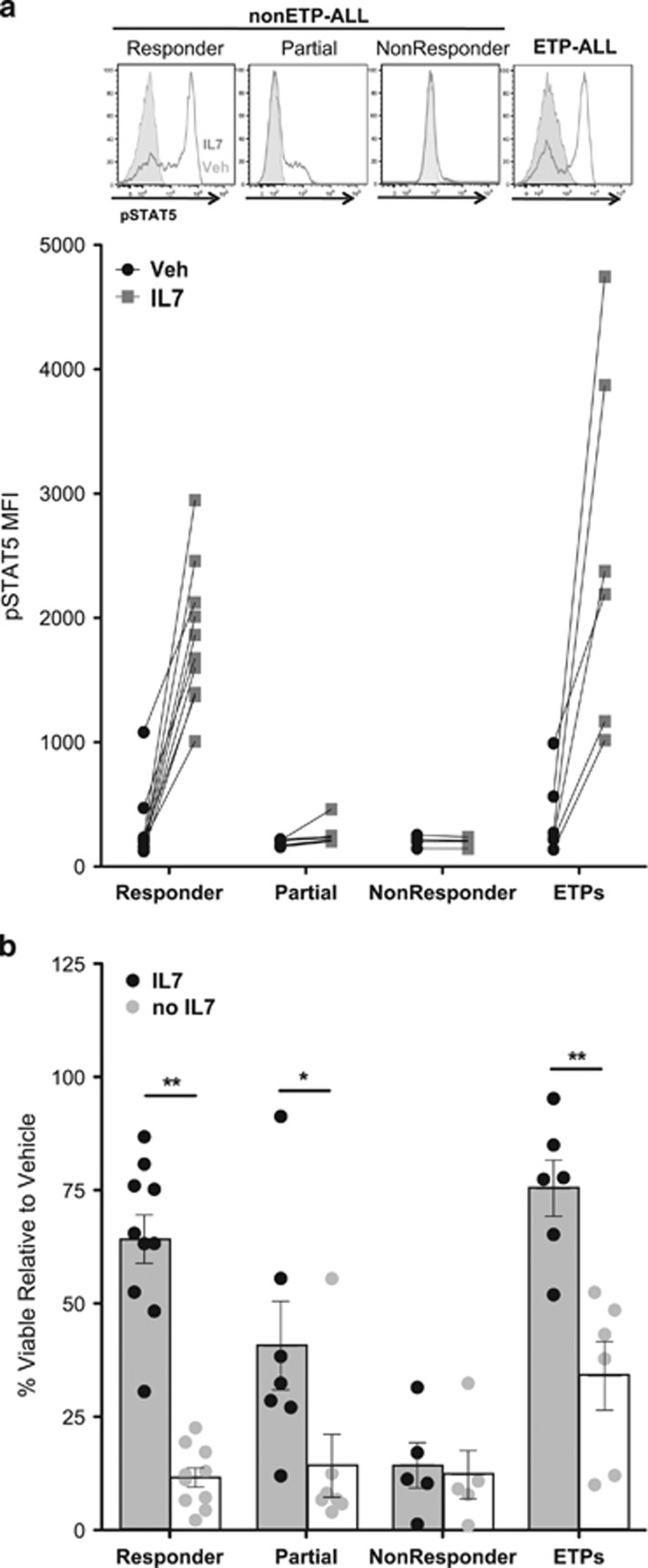
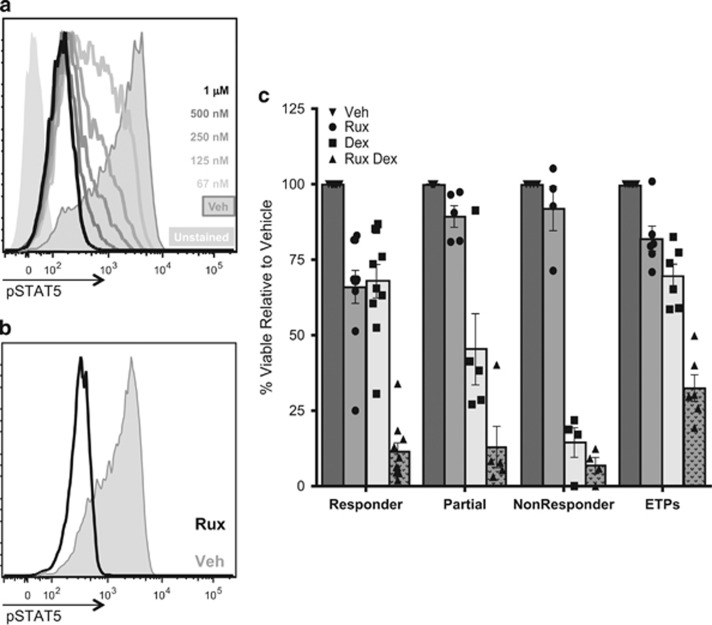
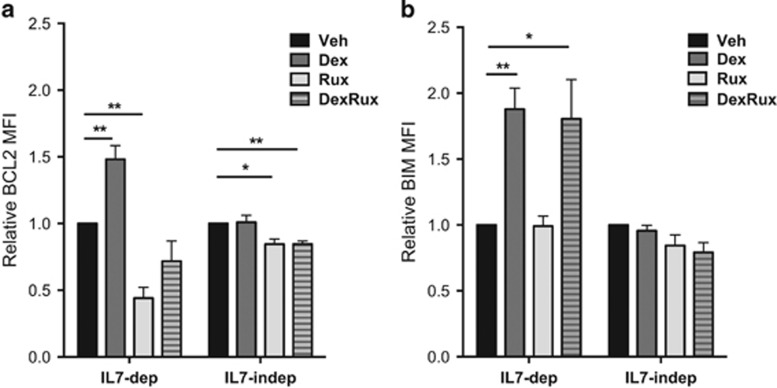
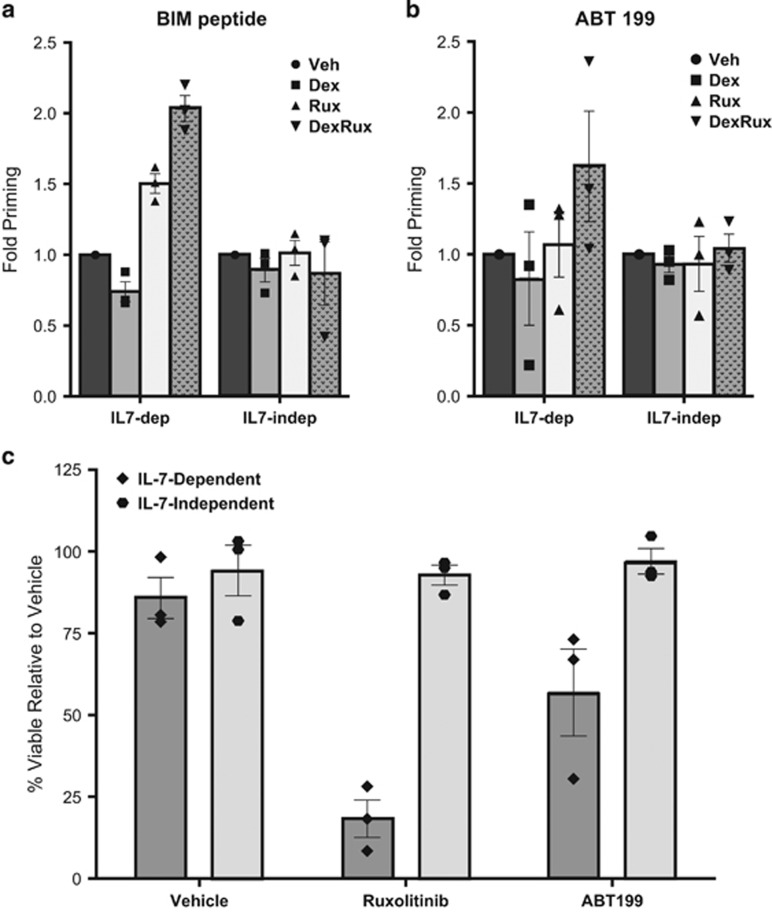
While outcomes for children with T-cell acute lymphoblastic leukemia (T-ALL) have improved dramatically, survival rates for patients with relapsed/refractory disease remain dismal. Prior studies indicate that glucocorticoid (GC) resistance is more common than resistance to other chemotherapies at relapse. In addition, failure to clear peripheral blasts during a prednisone prophase correlates with an elevated risk of relapse in newly diagnosed patients. Here we show that intrinsic GC resistance is present at diagnosis in early thymic precursor (ETP) T-ALLs as well as in a subset of non-ETP T-ALLs. GC-resistant non-ETP T-ALLs are characterized by strong induction of JAK/STAT signaling in response to interleukin-7 (IL7) stimulation. Removing IL7 or inhibiting JAK/STAT signaling sensitizes these T-ALLs, and a subset of ETP T-ALLs, to GCs. The combination of the GC dexamethasone and the JAK1/2 inhibitor ruxolitinib altered the balance between pro- and anti-apoptotic factors in samples with IL7-dependent GC resistance, but not in samples with IL7-independent GC resistance. Together, these data suggest that the addition of ruxolitinib or other inhibitors of IL7 receptor/JAK/STAT signaling may enhance the efficacy of GCs in a biologically defined subset of T-ALL.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Efficacy of JAK/STAT pathway inhibition in murine xenograft models of early T-cell precursor (ETP) acute lymphoblastic leukemia.Blood. 2015 Mar 12;125(11):1759-67. doi: 10.1182/blood-2014-06-580480. Epub 2015 Feb 2. Blood. 2015. PMID: 25645356 Free PMC article.
-
JAK/BCL2 inhibition acts synergistically with LSD1 inhibitors to selectively target ETP-ALL.Leukemia. 2022 Dec;36(12):2802-2816. doi: 10.1038/s41375-022-01716-9. Epub 2022 Oct 13. Leukemia. 2022. PMID: 36229595 Free PMC article.
-
Glucocorticoids paradoxically facilitate steroid resistance in T cell acute lymphoblastic leukemias and thymocytes.J Clin Invest. 2020 Feb 3;130(2):863-876. doi: 10.1172/JCI130189. J Clin Invest. 2020. PMID: 31687977 Free PMC article.
-
Targeting steroid resistance in T-cell acute lymphoblastic leukemia.Blood Rev. 2019 Nov;38:100591. doi: 10.1016/j.blre.2019.100591. Epub 2019 Jul 19. Blood Rev. 2019. PMID: 31353059 Review.
-
Molecular pathways: molecular basis for sensitivity and resistance to JAK kinase inhibitors.Clin Cancer Res. 2014 Apr 15;20(8):2051-9. doi: 10.1158/1078-0432.CCR-13-0279. Epub 2014 Feb 28. Clin Cancer Res. 2014. PMID: 24583800 Free PMC article. Review.
Cited by
-
Overcoming Glucocorticoid Resistance in Acute Lymphoblastic Leukemia: Repurposed Drugs Can Improve the Protocol.Front Oncol. 2021 Mar 11;11:617937. doi: 10.3389/fonc.2021.617937. eCollection 2021. Front Oncol. 2021. PMID: 33777761 Free PMC article. Review.
-
Models Contribution to the Understanding of Sarcoidosis Pathogenesis: "Are There Good Models of Sarcoidosis?".J Clin Med. 2020 Jul 31;9(8):2445. doi: 10.3390/jcm9082445. J Clin Med. 2020. PMID: 32751786 Free PMC article. Review.
-
Integrated bioinformatics analysis of the crucial candidate genes and pathways associated with glucocorticoid resistance in acute lymphoblastic leukemia.Cancer Med. 2020 Apr;9(8):2918-2929. doi: 10.1002/cam4.2934. Epub 2020 Feb 25. Cancer Med. 2020. PMID: 32096603 Free PMC article.
-
Beyond Corticoresistance, A Paradoxical Corticosensitivity Induced by Corticosteroid Therapy in Pediatric Acute Lymphoblastic Leukemias.Cancers (Basel). 2023 May 18;15(10):2812. doi: 10.3390/cancers15102812. Cancers (Basel). 2023. PMID: 37345151 Free PMC article. Review.
-
Prognostic significance of ETP phenotype and minimal residual disease in T-ALL: a Children's Oncology Group study.Blood. 2023 Dec 14;142(24):2069-2078. doi: 10.1182/blood.2023020678. Blood. 2023. PMID: 37556734 Free PMC article. Clinical Trial.
References
-
- Graux C, Cools J, Michaux L, Vandenberghe P, Hagemeijer A. Cytogenetics and molecular genetics of T-cell acute lymphoblastic leukemia: from thymocyte to lymphoblast. Leukemia 2006; 20: 1496–1510. - PubMed
-
- Bhojwani D, Pui C-H. Relapsed childhood acute lymphoblastic leukaemia. Lancet Oncol 2013; 14: e205–e217. - PubMed
-
- Dördelmann M, Reiter A, Borkhardt A, Ludwig WD, Götz N, Viehmann S et al. Prednisone response is the strongest predictor of treatment outcome in infant acute lymphoblastic leukemia. Blood 1999; 94: 1209–1217. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
