

Echocardiographic Evaluation of Pericardial Effusion and Cardiac Tamponade
- PMID: 28484689
- PMCID: PMC5401877
- DOI: 10.3389/fped.2017.00079
Echocardiographic Evaluation of Pericardial Effusion and Cardiac Tamponade
Abstract
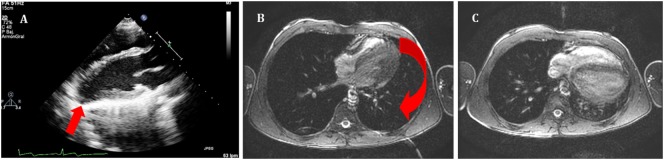
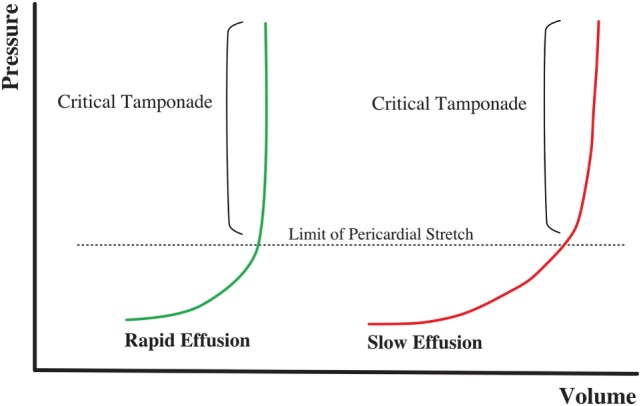
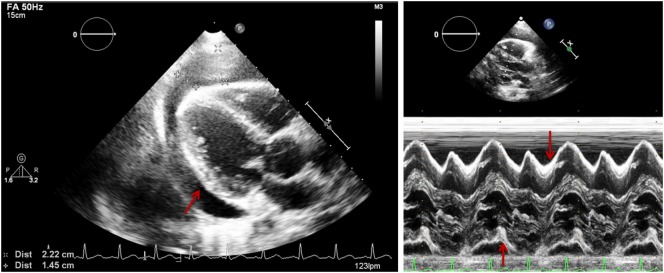
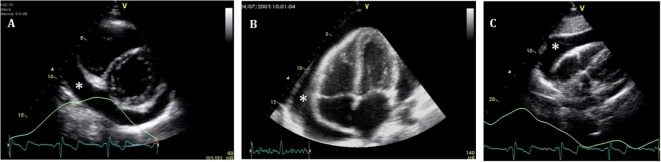
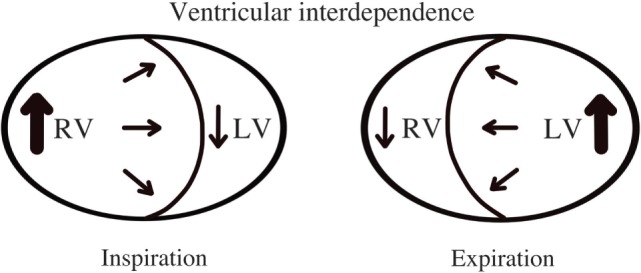
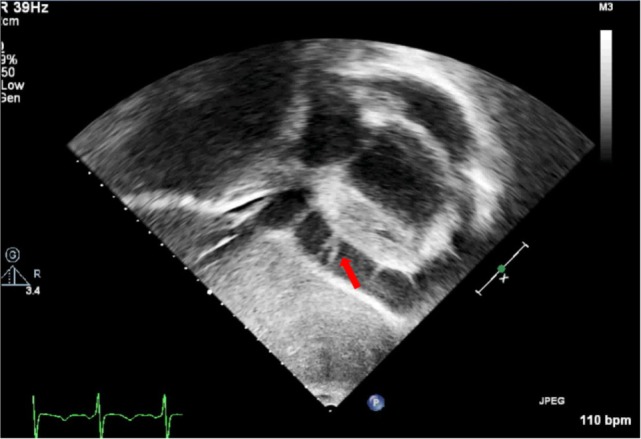
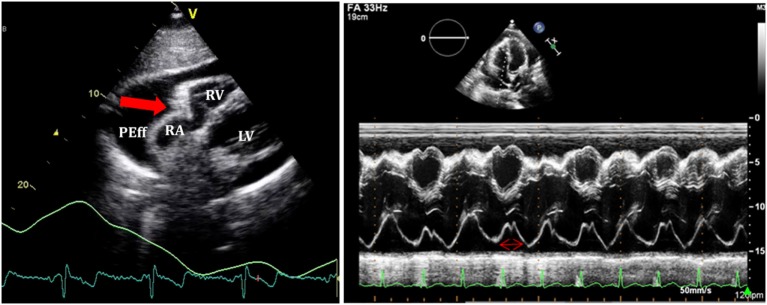
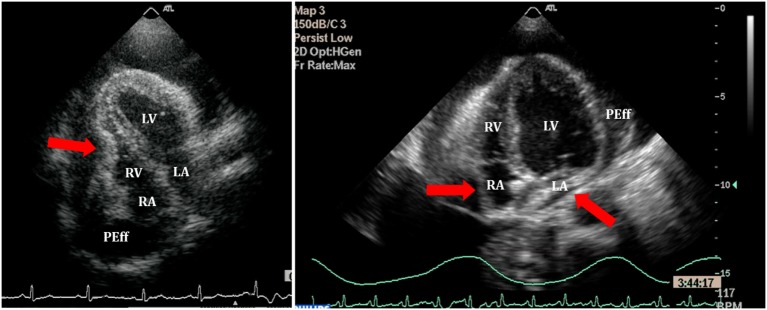
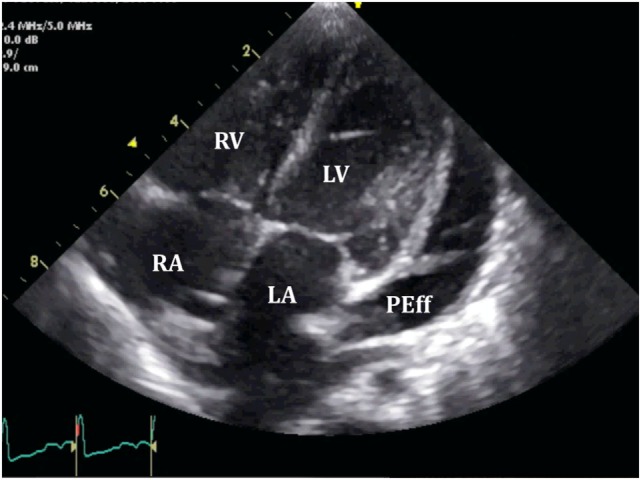
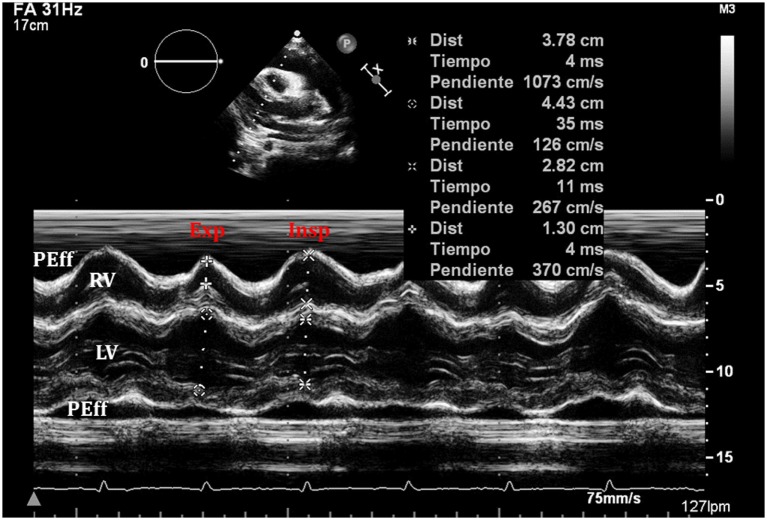
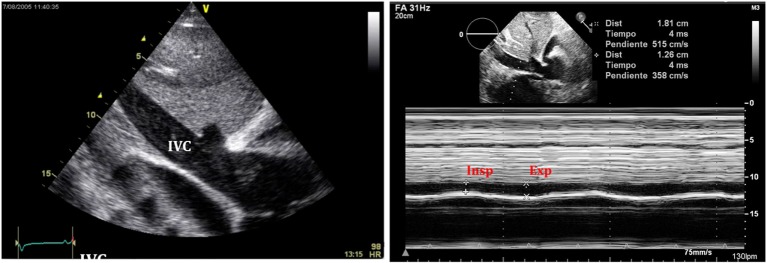
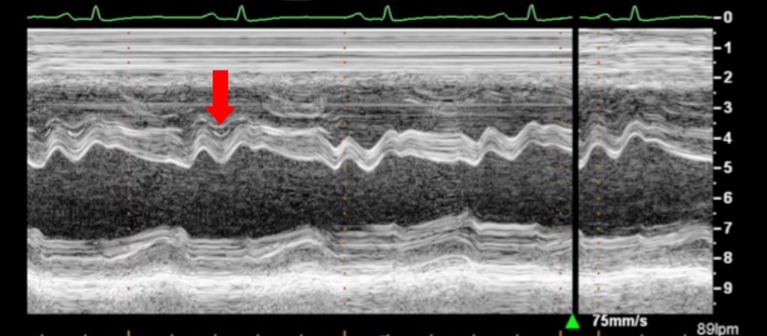
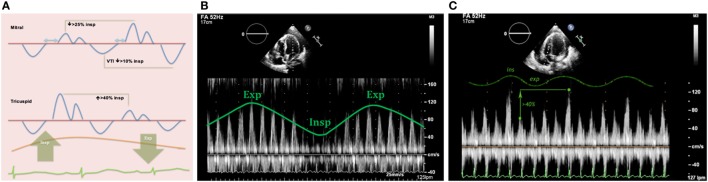
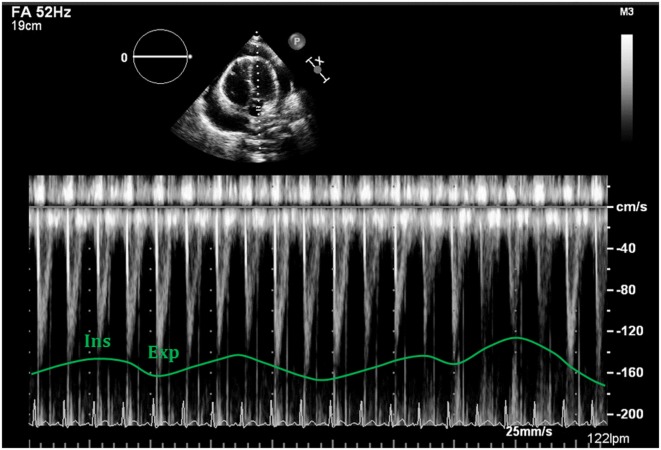
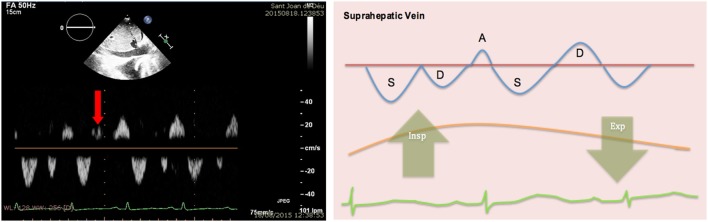
Pericardial effusion (PEff) is defined by an increase in the physiological amount of fluid within the pericardial space. It can appear following different medical conditions, mainly related to inflammation and cardiac surgery. Cardiac tamponade is a critical condition that occurs after sudden and/or excessive accumulation of fluid in the pericardial space that restricts appropriate filling of the cardiac chambers disturbing normal hemodynamics and ultimately causing hypotension and cardiac arrest. It is, therefore, a life-threatening condition that must be diagnosed as soon as possible for correct treatment and management. Echocardiographic evaluation of PEff is paramount for timely and appropriate diagnosis and management. A structured echocardiographic approach including two-dimensional, M-mode, and Doppler echocardiographic evaluation assessing (i) quantity and quality of pericardial fluid, (ii) collapse of cardiac chambers, (iii) respiratory variation of the ventricular diameters, (iv) inferior vena cava collapsibility, and (v) flow patterns in atrioventricular valves should give the bedside clinician the necessary information to appropriately manage PEff. Here, we review these key echocardiographic signs that will ensure an appropriate assessment of a patient with PEff and/or cardiac tamponade.
Keywords: cardiac tamponade; echocardiography; pericardial effusion; pericardium; ultrasound.
Figures
References
-
- Edler I. The diagnostic use of ultrasound in heart disease. Acta Med Scand Suppl (1955) 308:32.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources