

Ileocaecal and transverse colonic tuberculosis mimicking colonic malignancy - A case report
- PMID: 28486175
- PMCID: PMC5423344
- DOI: 10.1016/j.ijscr.2017.04.016
Ileocaecal and transverse colonic tuberculosis mimicking colonic malignancy - A case report
Abstract
Introduction: Gastrointestinal tuberculosis is common in the developing world especially in the lower socioeconomic groups. In elderly, it may mimic malignancy.
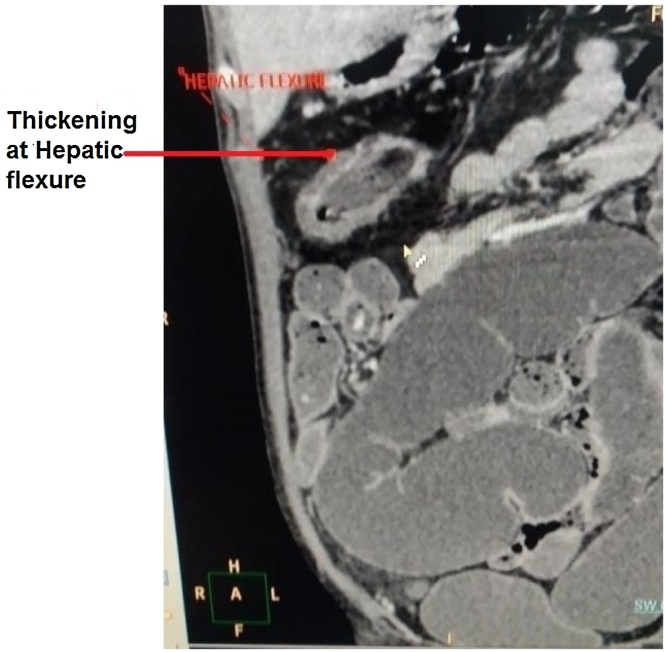
Case presentation: A 46-year-old female presented with a 6 month history of diffuse pain in abdomen with low grade fever and loss of weight and appetite. Clinically, differential of malignancy of the large bowel was considered. The computerized tomography(CT) scan of the abdomen revealed a diffuse concentric long segmental thickening of terminal ileum, ileo ceacal junction, ascending colon and narrowing of the transverse colonic end of the splenic flexure suggesting an infective etiology. Colonoscopy showed an ulcero-nodular lesion at the splenic flexure raising the possibility of colonic cancer and thickening of ascending colon and caecum. Colonoscopic biopsy from both sites, on histopathology, showed a moderate mixed inflammation and occasional lymphoid collection and crypt abscesses in the lamina propria giving a differential of tuberculosis or Crohn's disease. Biopsy smear showed occasional acid fast bacilli(AFBs) and the gene Xpert detected mycobacterium tuberculosis(MTB). The patient was started on anti Koch's therapy(AKT).
Discussion: In this case the differential diagnosis was malignancy of the colon, inflammatory bowel disease and tuberculosis as all these conditions may have similar clinical profile and radiological findings. Tuberculosis of bowel was considered as the most probable diagnosis due to the CT findings. But the colonoscopy suggested malignant etiology.
Conclusion: Possibility of tuberculosis should be kept in mind while dealing with synchronous lesions in large intestine.
Keywords: Case report; Colonic cancer; Crohn’s disease; Crypt abscess; Gastrointestinal tuberculosis; Inflammatory bowel disease.
Copyright © 2017 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures



References
-
- Horvath K.D., Whelan R.L. Intestinal tuberculosis: return of an old disease. Am. J. Gastroenterol. 1998;93:692–696. - PubMed
-
- Akhan O., Pringot J. Imaging of abdominal tuberculosis. Eur. Radiol. 2002;12:312–323. - PubMed
-
- Patel N., Amarapurkar D., Agal S., Baijal R., Kulshrestha P., Pramanik S. Gastrointestinal luminal tuberculosis: establishing the diagnosis. J. Gastroenterol. Hepatol. 2004;19:1240–1246. - PubMed
-
- Sharma R. Abdominal tuberculosis. Imaging Sci. Today. 2009;14:6. (Cited2016 Mar 31)
LinkOut - more resources
Full Text Sources
Other Literature Sources
