

Validation of the Vasoactive-Inotropic Score in Pediatric Sepsis
- PMID: 28486385
- PMCID: PMC5548505
- DOI: 10.1097/PCC.0000000000001191
Validation of the Vasoactive-Inotropic Score in Pediatric Sepsis
Abstract
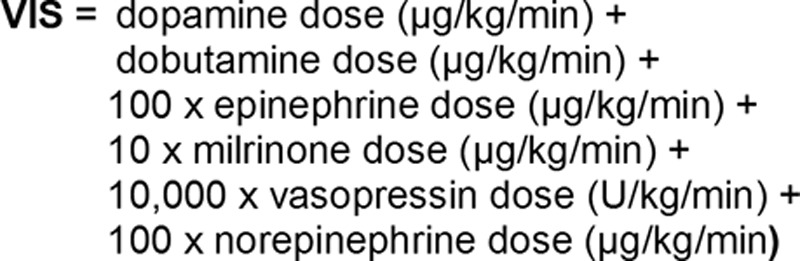
Objectives: To assess the validity of Vasoactive-Inotropic Score as a scoring system for cardiovascular support and surrogate outcome in pediatric sepsis.
Design: Secondary retrospective analysis of a single-center sepsis registry.
Setting: Freestanding children's hospital and tertiary referral center.
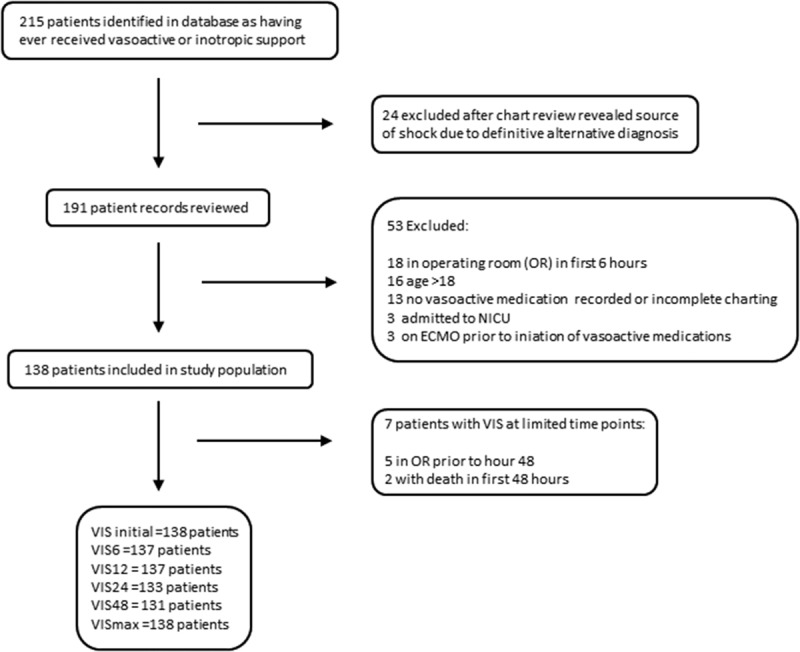
Patients: Children greater than 60 days and less than 18 years with sepsis identified in the emergency department between January 2012 and June 2015 treated with at least one vasoactive medication within 48 hours of admission to the PICU.
Interventions: None.
Measurements and main results: Vasoactive-Inotropic Score was abstracted at 6, 12, 24, and 48 hours post ICU admission. Primary outcomes were ventilator days and ICU length of stay. The secondary outcome was a composite outcome of cardiac arrest/extracorporeal membrane oxygenation/in-hospital mortality. One hundred thirty-eight patients met inclusion criteria. Most common infectious sources were pneumonia (32%) and bacteremia (23%). Thirty-three percent were intubated and mortality was 6%. Of the time points assessed, Vasoactive-Inotropic Score at 48 hours showed the strongest correlation with ICU length of stay (r = 0.53; p < 0.0001) and ventilator days (r = 0.52; p < 0.0001). On multivariable analysis, Vasoactive-Inotropic Score at 48 hours was a strong independent predictor of primary outcomes and intubation. For every unit increase in Vasoactive-Inotropic Score at 48 hours, there was a 13% increase in ICU length of stay (p < 0.001) and 8% increase in ventilator days (p < 0.01). For every unit increase in Vasoactive-Inotropic Score at 12 hours, there was a 14% increase in odds of having the composite outcome (p < 0.01).
Conclusions: Vasoactive-Inotropic Score in pediatric sepsis patients is independently associated with important clinically relevant outcomes including ICU length of stay, ventilator days, and cardiac arrest/extracorporeal membrane oxygenation/mortality. Vasoactive-Inotropic Score may be a useful surrogate outcome in pediatric sepsis.
Conflict of interest statement
Dr. Davidson received support for article research from the National Institutes of Health (NIH), and his institution received funding from NIH/National Heart, Lung, and Blood Institute K23. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Outcome Measures in Sepsis, Revisited.Pediatr Crit Care Med. 2017 Aug;18(8):803-804. doi: 10.1097/PCC.0000000000001209. Pediatr Crit Care Med. 2017. PMID: 28796705 No abstract available.
-
Vasoactive-Inotropic Score: Is It Reliable in Pediatric Sepsis as a Predictive Outcome Measure?Pediatr Crit Care Med. 2017 Oct;18(10):1003. doi: 10.1097/PCC.0000000000001270. Pediatr Crit Care Med. 2017. PMID: 28976471 No abstract available.
-
The authors reply.Pediatr Crit Care Med. 2017 Oct;18(10):1003-1005. doi: 10.1097/PCC.0000000000001283. Pediatr Crit Care Med. 2017. PMID: 28976472 Free PMC article. No abstract available.
References
-
- Hartman ME, Linde-Zwirble WT, Angus DC, et al. Trends in the epidemiology of pediatric severe sepsis. Pediatr Crit Care Med 2013; 14:686–693 - PubMed
-
- Weiss SL, Fitzgerald JC, Maffei FA, et al. SPROUT Study Investigators and Pediatric Acute Lung Injury and Sepsis Investigators Network: Discordant identification of pediatric severe sepsis by research and clinical definitions in the SPROUT international point prevalence study. Crit Care 2015; 19:325. - PMC - PubMed
-
- Goldstein B, Giroir B, Randolph AMembers of the International Consensus Conference on Pediatric Sepsis: International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 2005; 6:2–8 - PubMed
-
- Carcillo JA, Kuch BA, Han YY, et al. Mortality and functional morbidity after use of PALS/APLS by community physicians. Pediatrics 2009; 124:500–508 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
