

Long-term inpatient disease burden in the Adult Life after Childhood Cancer in Scandinavia (ALiCCS) study: A cohort study of 21,297 childhood cancer survivors
- PMID: 28486495
- PMCID: PMC5423554
- DOI: 10.1371/journal.pmed.1002296
Long-term inpatient disease burden in the Adult Life after Childhood Cancer in Scandinavia (ALiCCS) study: A cohort study of 21,297 childhood cancer survivors
Abstract
Background: Survivors of childhood cancer are at increased risk for a wide range of late effects. However, no large population-based studies have included the whole range of somatic diagnoses including subgroup diagnoses and all main types of childhood cancers. Therefore, we aimed to provide the most detailed overview of the long-term risk of hospitalisation in survivors of childhood cancer.
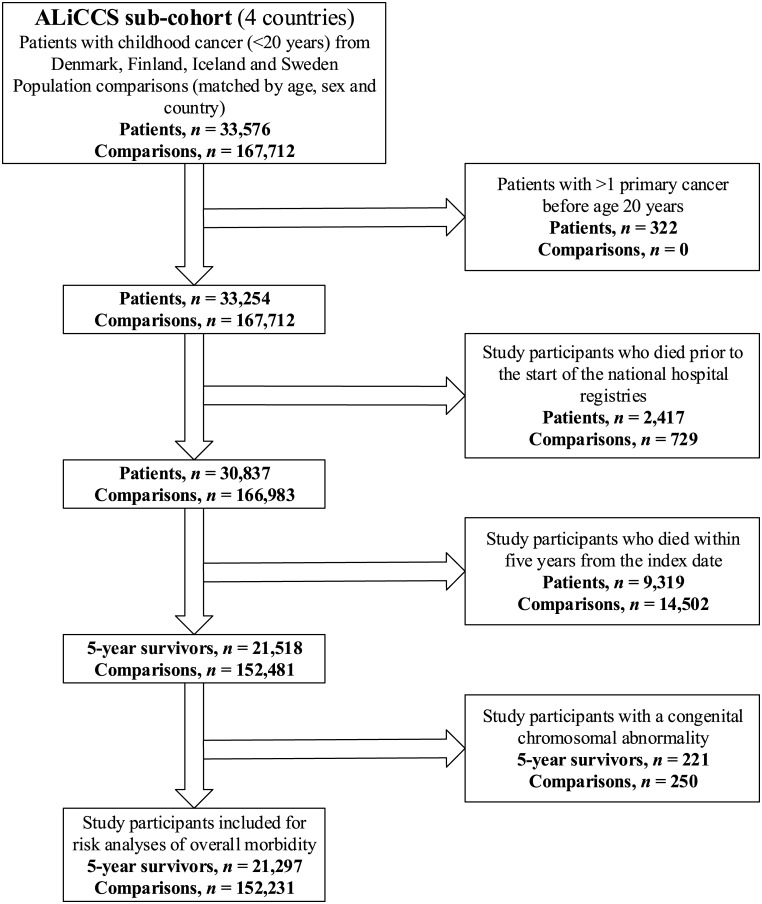
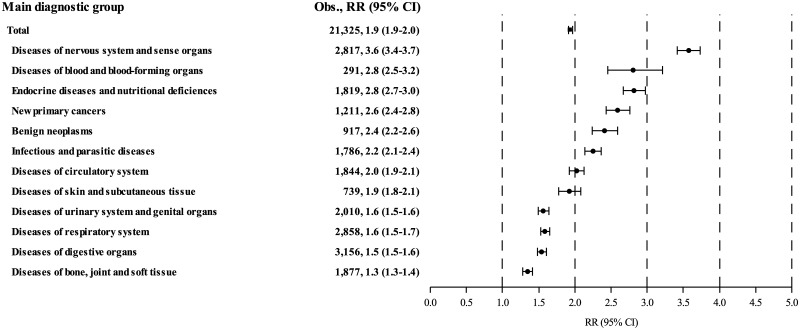
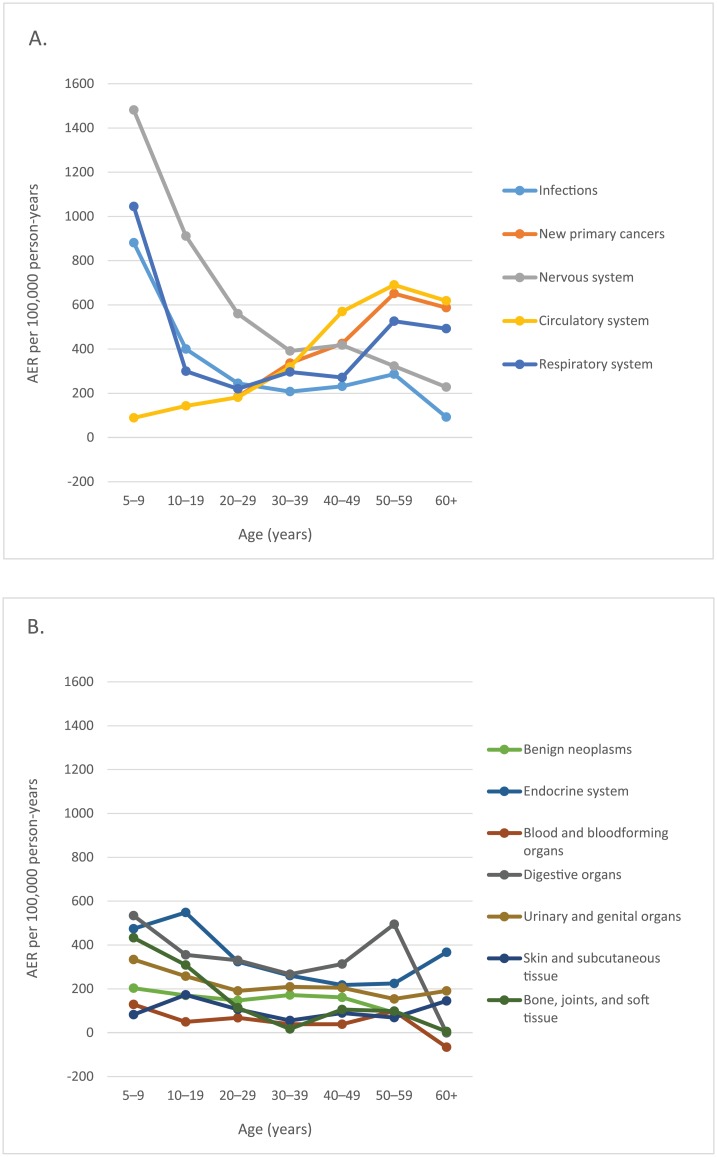
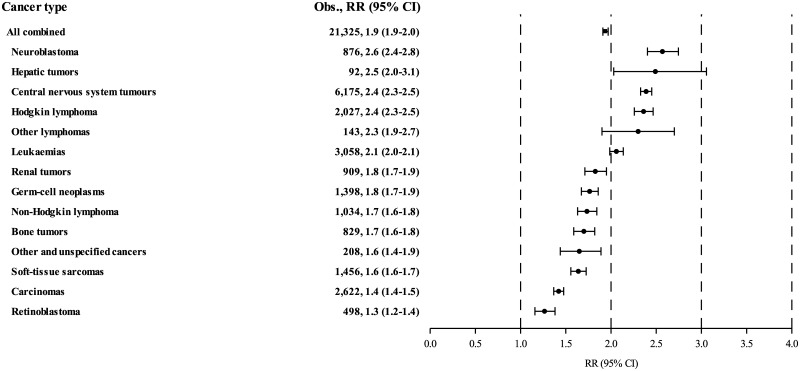
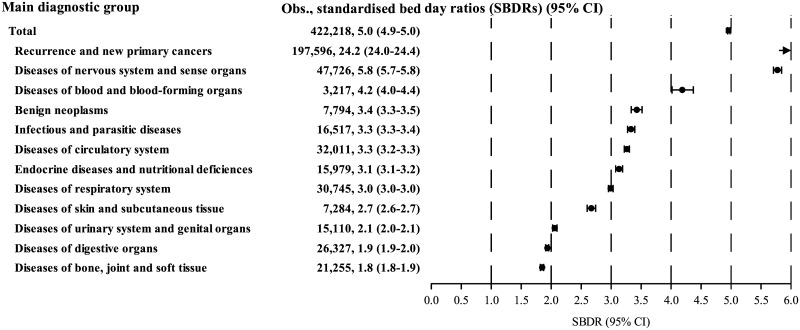
Methods and findings: From the national cancer registers of Denmark, Finland, Iceland, and Sweden, we identified 21,297 5-year survivors of childhood cancer diagnosed with cancer before the age of 20 years in the periods 1943-2008 in Denmark, 1971-2008 in Finland, 1955-2008 in Iceland, and 1958-2008 in Sweden. We randomly selected 152,231 population comparison individuals matched by age, sex, year, and country (or municipality in Sweden) from the national population registers. Using a cohort design, study participants were followed in the national hospital registers in Denmark, 1977-2010; Finland, 1975-2012; Iceland, 1999-2008; and Sweden, 1968-2009. Disease-specific hospitalisation rates in survivors and comparison individuals were used to calculate survivors' standardised hospitalisation rate ratios (RRs), absolute excess risks (AERs), and standardised bed day ratios (SBDRs) based on length of stay in hospital. We adjusted for sex, age, and year by indirect standardisation. During 336,554 person-years of follow-up (mean: 16 years; range: 0-42 years), childhood cancer survivors experienced 21,325 first hospitalisations for diseases in one or more of 120 disease categories (cancer recurrence not included), when 10,999 were expected, yielding an overall RR of 1.94 (95% confidence interval [95% CI] 1.91-1.97). The AER was 3,068 (2,980-3,156) per 100,000 person-years, meaning that for each additional year of follow-up, an average of 3 of 100 survivors were hospitalised for a new excess disease beyond the background rates. Approximately 50% of the excess hospitalisations were for diseases of the nervous system (19.1% of all excess hospitalisations), endocrine system (11.1%), digestive organs (10.5%), and respiratory system (10.0%). Survivors of all types of childhood cancer were at increased, persistent risk for subsequent hospitalisation, the highest risks being those of survivors of neuroblastoma (RR: 2.6 [2.4-2.8]; n = 876), hepatic tumours (RR: 2.5 [2.0-3.1]; n = 92), central nervous system tumours (RR: 2.4 [2.3-2.5]; n = 6,175), and Hodgkin lymphoma (RR: 2.4 [2.3-2.5]; n = 2,027). Survivors spent on average five times as many days in hospital as comparison individuals (SBDR: 4.96 [4.94-4.98]; n = 422,218). The analyses of bed days in hospital included new primary cancers and recurrences. Of the total 422,218 days survivors spent in hospital, 47% (197,596 bed days) were for new primary cancers and recurrences. Our study is likely to underestimate the absolute overall disease burden experienced by survivors, as less severe late effects are missed if they are treated sufficiently in the outpatient setting or in the primary health care system.
Conclusions: Childhood cancer survivors were at increased long-term risk for diseases requiring inpatient treatment even decades after their initial cancer. Health care providers who do not work in the area of late effects, especially those in primary health care, should be aware of this highly challenged group of patients in order to avoid or postpone hospitalisations by prevention, early detection, and appropriate treatments.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- de Nully BP, Olsen JH, Hertz H, Carstensen B, Bautz A. Trends in survival after childhood cancer in Denmark, 1943–87: a population-based study. Acta Paediatr. 1995;84(3):316–24. - PubMed
-
- de Fine Licht S, Winther JF, Gudmundsdottir T, Holmqvist AS, Bonnesen TG, Asdahl PH, et al. Hospital contacts for endocrine disorders in Adult Life after Childhood Cancer in Scandinavia (ALiCCS): a population-based cohort study. Lancet. 2014;383(9933):1981–9. 10.1016/S0140-6736(13)62564-7 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
