

Angle stability and outflow in dual blade ab interno trabeculectomy with active versus passive chamber management
- PMID: 28486513
- PMCID: PMC5423641
- DOI: 10.1371/journal.pone.0177238
Angle stability and outflow in dual blade ab interno trabeculectomy with active versus passive chamber management
Abstract
Purpose: To compare intraoperative angle stability and postoperative outflow of two ab interno trabeculectomy devices that excise the trabecular meshwork with or without active aspiration and irrigation. We hypothesized that anterior segment optical coherence tomography (AS-OCT) allows for a quantitative comparison of intraoperative angle stability in a microincisional glaucoma surgery (MIGS) pig eye training model.
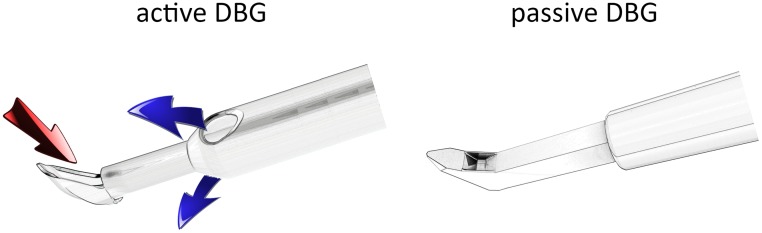
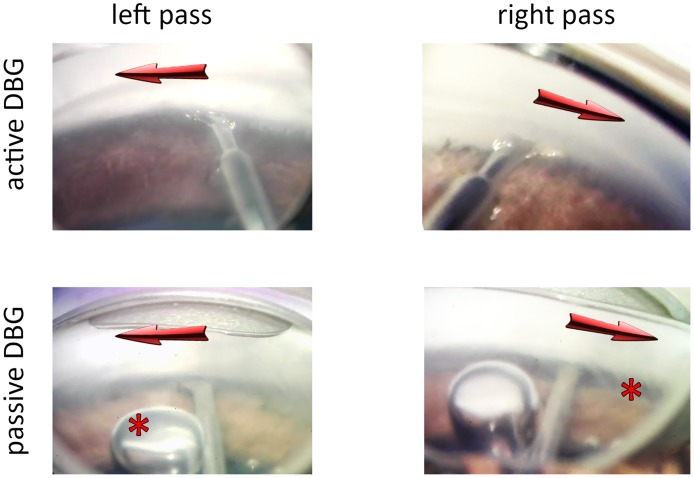
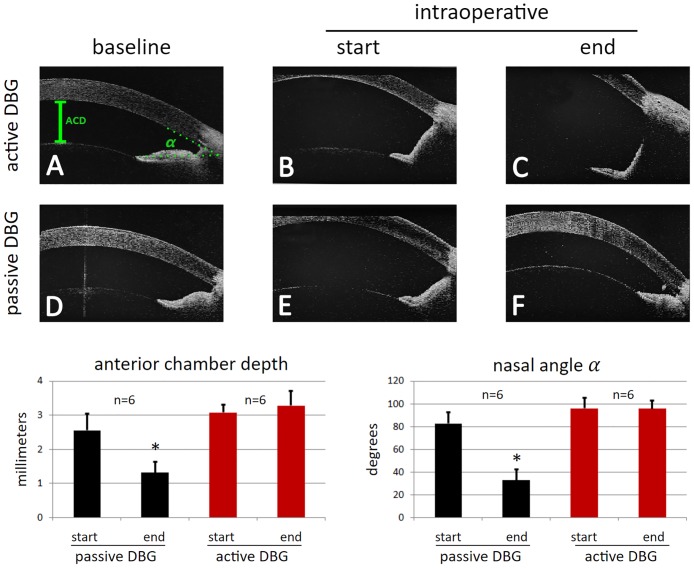
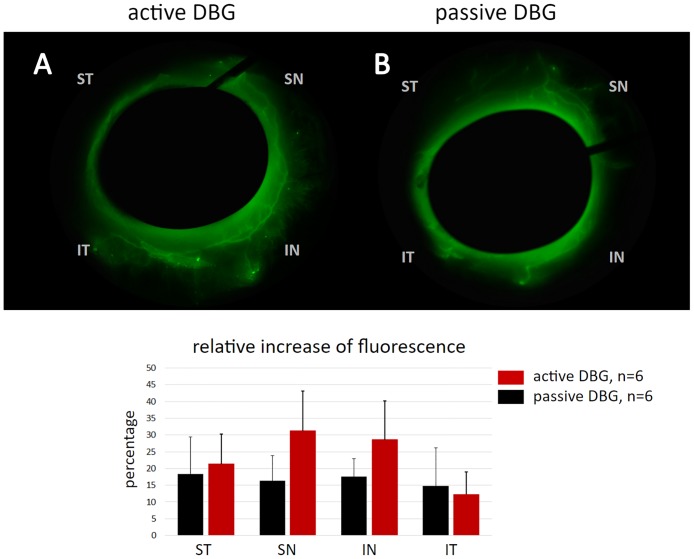
Methods: Twelve freshly enucleated porcine eyes were measured with AS-OCT at baseline, at the beginning of the procedure and at its conclusion to determine the anterior chamber depth (ACD) and the nasal angle α in degrees. The right and left eye of pairs were randomly assigned to an active dual blade goniectome (aDBG) and a passive dual blade goniectome (pDBG) group, respectively. The aDBG had irrigation and aspiration ports while the pDBG required surgery under viscoelastic. We performed the procedures using our MIGS training system with a standard, motorized ophthalmic operating microscope. We estimated outflow by obtaining canalograms with fluorescent spheres.
Results: In aDBG, the nasal angle remained wide open during the procedure at above 90° and did not change towards the end (100±10%, p = 0.9). In contrast, in pDBG, ACD decreased by 51±19% to 21% below baseline (p<0.01) while the angle progressively narrowed by 40±12% (p<0.001). Canalograms showed a similar extent of access to the outflow tract with the aDBG and the pDBG (p = 0.513). The average increase for the aDBG in the superonasal and inferonasal quadrants was between 27 to 31% and for the pDBG between 15 to 18%.
Conclusion: AS-OCT demonstrated that active irrigation and aspiration improved anterior chamber maintenance and ease of handling with the aDBG in this MIGS training model. The immediate postoperative outflow was equally good with both devices.
Conflict of interest statement
Figures
References
-
- Kaplowitz K, Loewen NA. Minimally Invasive and Nonpenetrating Glaucoma Surgery In: Yanoff M, DJ S., editors. Ophthalmology: Expert Consult. Elsevier; 2013. pp. 1133–1146.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
