

Burst-suppression ratio underestimates absolute duration of electroencephalogram suppression compared with visual analysis of intraoperative electroencephalogram
- PMID: 28486575
- PMCID: PMC6224027
- DOI: 10.1093/bja/aex054
Burst-suppression ratio underestimates absolute duration of electroencephalogram suppression compared with visual analysis of intraoperative electroencephalogram
Abstract
Background: Machine-generated indices based on quantitative electroencephalography (EEG), such as the patient state index (PSI™) and burst-suppression ratio (BSR), are increasingly being used to monitor intraoperative depth of anaesthesia in the endeavour to improve postoperative neurological outcomes, such as postoperative delirium (POD). However, the accuracy of the BSR compared with direct visualization of the EEG trace with regard to the prediction of POD has not been evaluated previously.
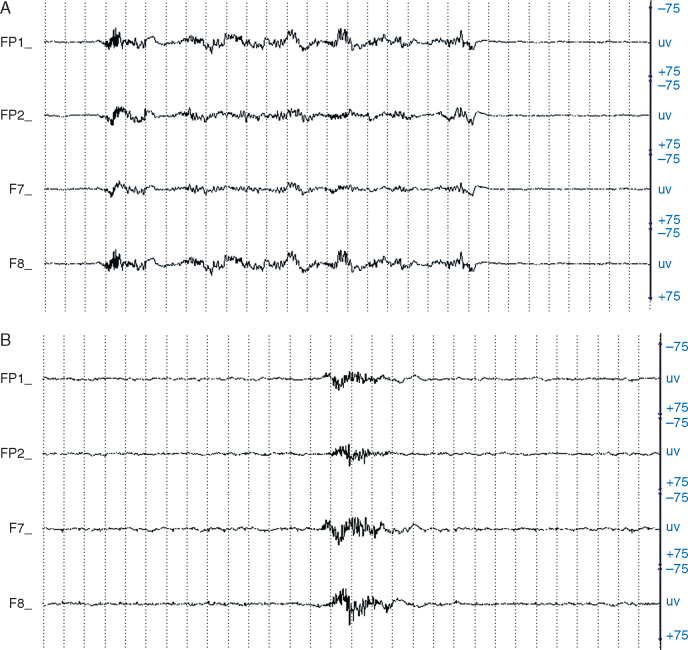
Methods: Forty-one consecutive patients undergoing non-cardiac, non-intracranial surgery with general anaesthesia wore a SedLine ® monitor during surgery and were assessed after surgery for the presence of delirium with the Confusion Assessment Method. The intraoperative EEG was scanned for absolute minutes of EEG suppression and correlated with the incidence of POD. The BSR and PSI™ were compared between patients with and without POD.
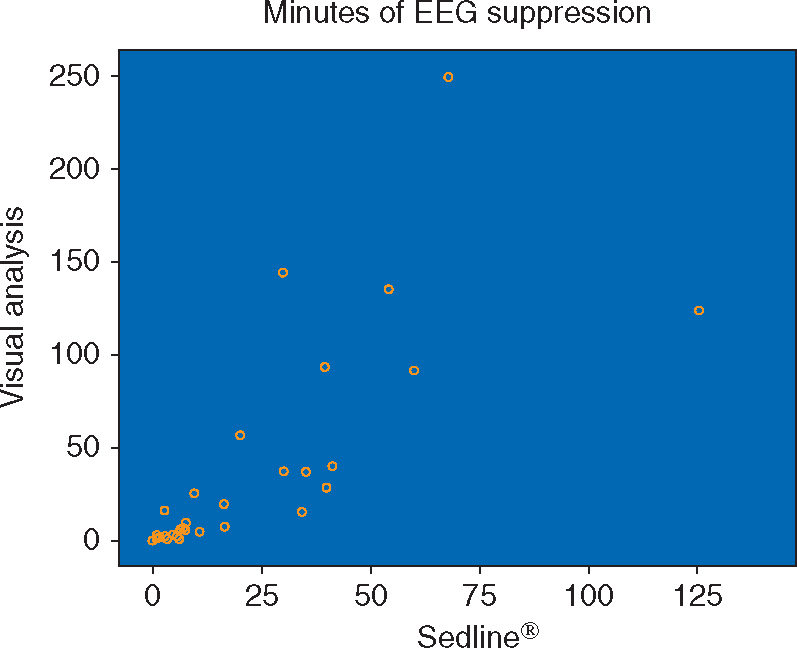
Results: Visual analysis of the EEG by neurologists and the SedLine ® -generated BSR provided a significantly different distribution of estimated minutes of EEG suppression ( P =0.037). The Sedline ® system markedly underestimated the amount of EEG suppression. The number of minutes of suppression assessed by visual analysis of the EEG was significantly associated with POD ( P =0.039), whereas the minutes based on the BSR generated by SedLine ® were not associated with POD ( P =0.275).
Conclusions: Our findings suggest that SedLine ® (machine)-generated indices might underestimate the minutes of EEG suppression, thereby reducing the sensitivity for detecting patients at risk for POD. Thus, the monitoring of machine-generated BSR and PSI™ might benefit from the addition of a visual tracing of the EEG to achieve a more accurate and real-time guidance of anaesthesia depth monitoring and the ultimate goal, to reduce the risk of POD.
Keywords: burst-suppression ratio; confusion assessment method; depth of anaesthesia; patient state index; postoperative delirium.
© The Author 2017. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: journals.permissions@oup.com
Figures
References
-
- Bin Abd Razak HR, Yung WYA. Postoperative delirium in patients undergoing total joint arthroplasty: a systematic review. J Arthroplasty. 2015;30:1414–1417. - PubMed
-
- Mashour GA, Woodrum DT, Avidan MS. Neurological complications of surgery and anaesthesia. Br J Anaesth. 2015;114:194–203. - PubMed
-
- Bilotta F, Lauretta MP, Borozdina A, Mizikov VM, Rosa G. Postoperative delirium: risk factors, diagnosis and perioperative care. Minerva Anestesiol. 2013;79:1066–1076. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
