

Clinical Identification of Oncogenic Drivers and Copy-Number Alterations in Pituitary Tumors
- PMID: 28486603
- PMCID: PMC5505210
- DOI: 10.1210/en.2016-1967
Clinical Identification of Oncogenic Drivers and Copy-Number Alterations in Pituitary Tumors
Abstract
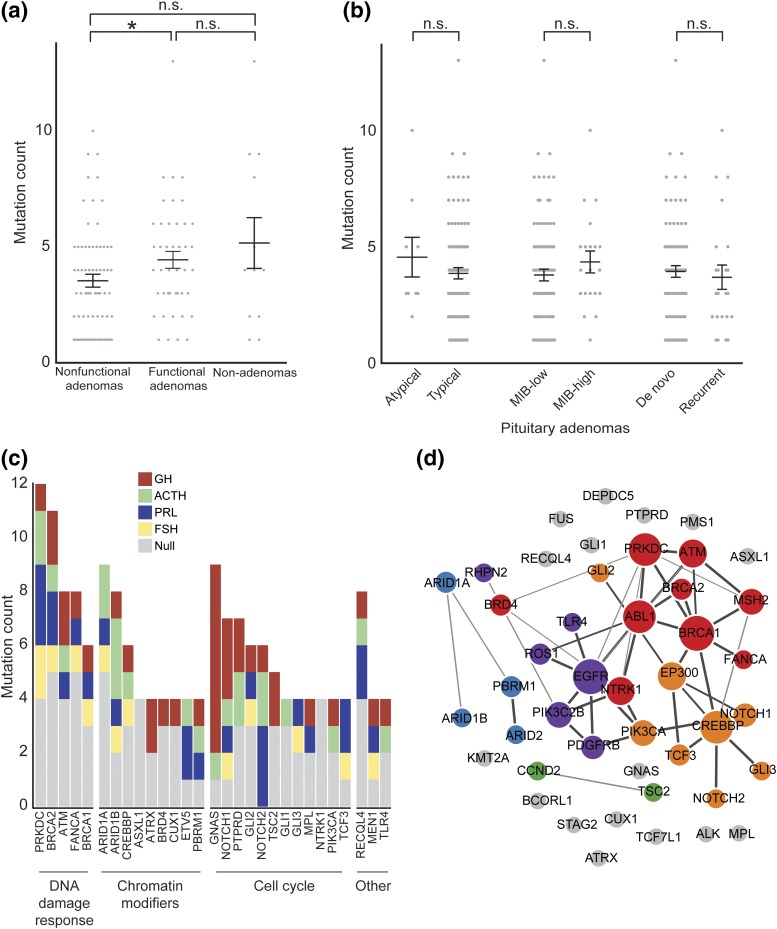
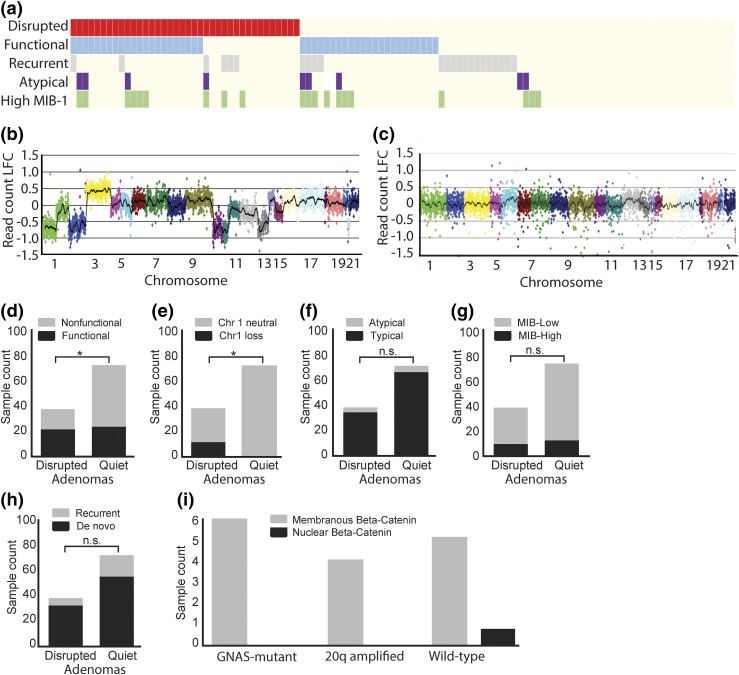
Pituitary tumors are the second most common adult primary brain tumor, with a variable clinical course. Recent work has identified a number of genetic determinants of pituitary tumor subtypes, which may augment traditional histopathologic classification schemes. We sought to determine whether pituitary tumors could be stratified based on objective molecular characteristics using a clinical genomics assay. We performed a retrospective analysis of patients operated on at the Brigham and Women's Hospital from 2012 to 2016 whose pituitary tumors were profiled using multiplexed next-generation sequencing. We analyzed 127 pituitary tumors, including 114 adenomas, 5 craniopharyngiomas, and 8 tumors of other histologies. We observed recurrent BRAFV600E mutations in papillary craniopharyngiomas, CTNNB1 mutations in adamantinomatous craniopharyngiomas, and activating GNAS mutations in growth hormone-secreting adenomas. Furthermore, we validated the presence of two distinct genomic subclasses in adenomas (i.e., those with disrupted or quiet copy-number profiles) and the significant association of disruption with functional hormone status (P < 0.05). We report the clinical implementation of next-generation sequencing of pituitary tumors. We confirmed previously identified molecular subclasses for these tumors and show that routine screening as part of clinical practice is both feasible and informative. This large-scale proof-of-principle study may help to guide future institutional efforts for pituitary tumor classification as well as the incorporation of such techniques into prospective analysis as part of clinical trials.
Copyright © 2017 Endocrine Society.
Figures
References
-
- de Aguiar PH, Aires R, Laws ER, Isolan GR, Logullo A, Patil C, Katznelson L. Labeling index in pituitary adenomas evaluated by means of MIB-1: is there a prognostic role? A critical review. Neurol Res. 2010;32(10):1060–1071. - PubMed
-
- Zaidi HA, Cote DJ, Dunn IF, Laws ER Jr. Predictors of aggressive clinical phenotype among immunohistochemically confirmed atypical adenomas. J Clin Neurosci. 2016;34:246–251. - PubMed
-
- Northcott PA, Korshunov A, Pfister SM, Taylor MD. The clinical implications of medulloblastoma subgroups. Nat Rev Neurol. 2012;8(6):340–351. - PubMed
-
- Witt H, Mack SC, Ryzhova M, Bender S, Sill M, Isserlin R, Benner A, Hielscher T, Milde T, Remke M, Jones DT, Northcott PA, Garzia L, Bertrand KC, Wittmann A, Yao Y, Roberts SS, Massimi L, Van Meter T, Weiss WA, Gupta N, Grajkowska W, Lach B, Cho YJ, von Deimling A, Kulozik AE, Witt O, Bader GD, Hawkins CE, Tabori U, Guha A, Rutka JT, Lichter P, Korshunov A, Taylor MD, Pfister SM. Delineation of two clinically and molecularly distinct subgroups of posterior fossa ependymoma. Cancer Cell. 2011;20(2):143–157. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
