

Mediation of the effect of malaria in pregnancy on stillbirth and neonatal death in an area of low transmission: observational data analysis
- PMID: 28486979
- PMCID: PMC5424335
- DOI: 10.1186/s12916-017-0863-z
Mediation of the effect of malaria in pregnancy on stillbirth and neonatal death in an area of low transmission: observational data analysis
Abstract
Background: Malaria in pregnancy is preventable and contributes significantly to the estimated 5.5 million stillbirths and neonatal deaths that occur annually. The contribution of malaria in pregnancy in areas of low transmission has not been quantified, and the roles of maternal anaemia, small-for-gestational-age status, and preterm birth in mediating the effect of malaria in pregnancy on stillbirth and neonatal death are poorly elucidated.
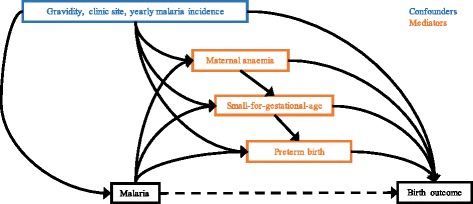
Methods: We analysed observational data routinely collected at antenatal clinics on the Thai-Myanmar border (1986-2015). We used Cox regression and sequential mediation analysis to determine the effect of falciparum and vivax malaria in pregnancy on antepartum (death in utero) and intrapartum (death during labour) stillbirth and neonatal mortality as well as mediation through maternal anaemia, preterm birth, and small-for-gestational-age status.
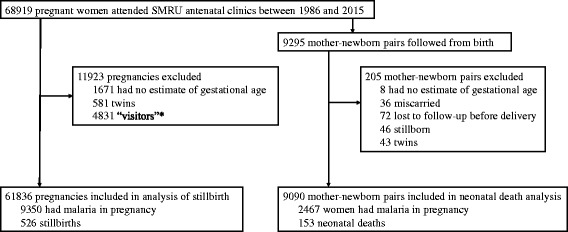
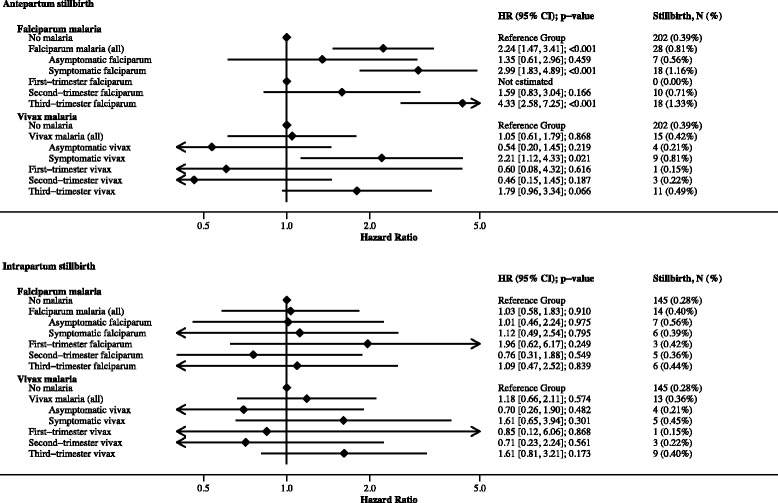
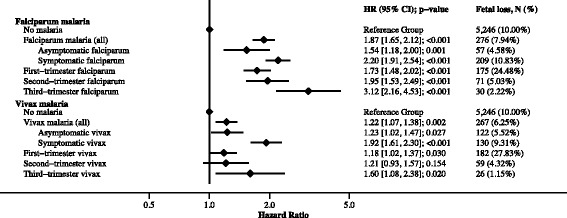
Results: Of 61,836 women, 9350 (15%) had malaria in pregnancy, and 526 (0.8%) had stillbirths. In a sub-set of 9090 live born singletons followed from birth there were 153 (1.7%) neonatal deaths. The hazard of antepartum stillbirth increased 2.24-fold [95% confidence interval: 1.47, 3.41] following falciparum malaria (42% mediated through small-for-gestational-age status and anaemia), driven by symptomatic falciparum malaria (hazard ratio, HR: 2.99 [1.83, 4.89]) rather than asymptomatic falciparum malaria (HR: 1.35 [0.61, 2.96]). The hazard of antepartum stillbirth increased 2.21-fold [1.12, 4.33] following symptomatic vivax malaria (24% mediated through small-for-gestational-age status and anaemia) but not asymptomatic vivax malaria (HR: 0.54 [0.20, 1.45]). There was no association between falciparum or vivax malaria in pregnancy and intrapartum stillbirth (falciparum HR: 1.03 [0.58, 1.83]; vivax HR: 1.18 [0.66, 2.11]). Falciparum and vivax malaria in pregnancy increased the hazard of neonatal death 2.55-fold [1.54, 4.22] and 1.98-fold [1.10, 3.57], respectively (40% and 50%, respectively, mediated through small-for-gestational-age status and preterm birth).
Conclusions: Prevention of malaria in pregnancy, new and existing interventions to prevent small-for-gestational-age status and maternal anaemia, and improved capacity for managing preterm and small-for-gestational-age newborns will reduce the number of malaria-associated stillbirths and neonatal deaths in malaria-endemic areas.
Keywords: Malaria in pregnancy; Mediation analysis; Neonatal death; Stillbirth.
Figures
References
-
- Blencowe H, Cousens S, Jassir FB, Say L, Chou D, Mathers C, et al. National, regional, and worldwide estimates of stillbirth rates in 2009 with trends since 1995: A systematic analysis. Lancet. 2016;377(9774):1319–30. - PubMed
-
- UN Inter-agency Group for Child Mortality Estimation . Levels and trends in child mortality: Report 2013. New York: UN Inter-agency Group for Child Mortality Estimation; 2013.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
