

A Multicenter, Randomized Trial of Ramped Position vs Sniffing Position During Endotracheal Intubation of Critically Ill Adults
- PMID: 28487139
- PMCID: PMC5812765
- DOI: 10.1016/j.chest.2017.03.061
A Multicenter, Randomized Trial of Ramped Position vs Sniffing Position During Endotracheal Intubation of Critically Ill Adults
Abstract
Background: Hypoxemia is the most common complication during endotracheal intubation of critically ill adults. Intubation in the ramped position has been hypothesized to prevent hypoxemia by increasing functional residual capacity and decreasing the duration of intubation, but has never been studied outside of the operating room.
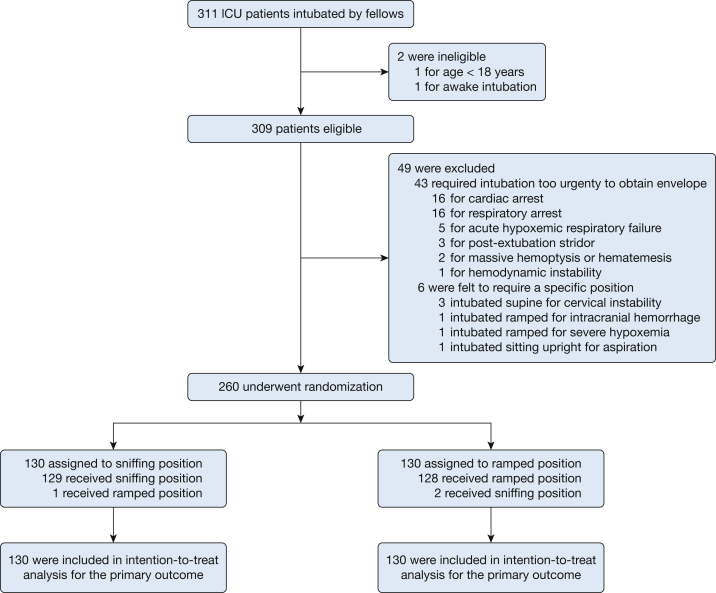
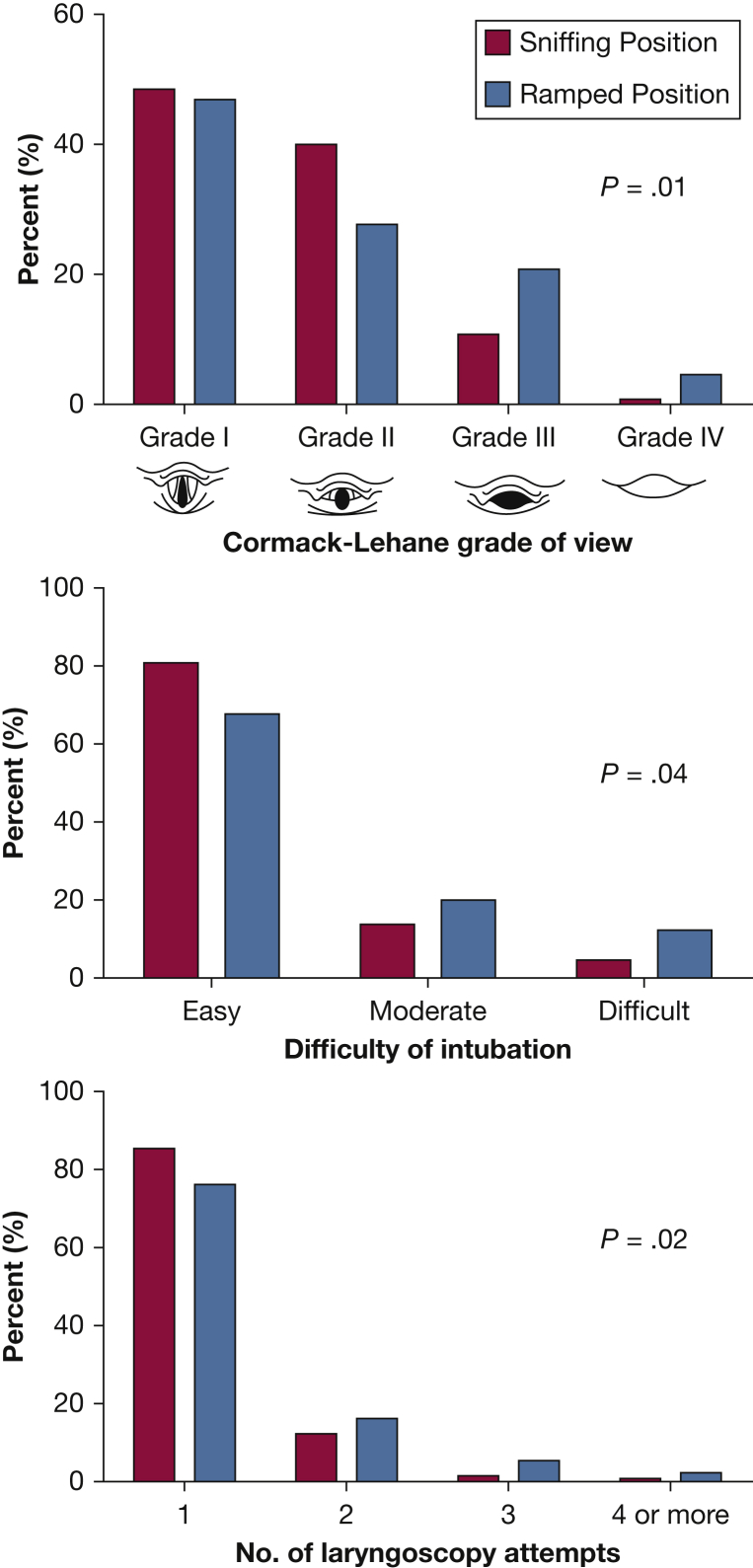
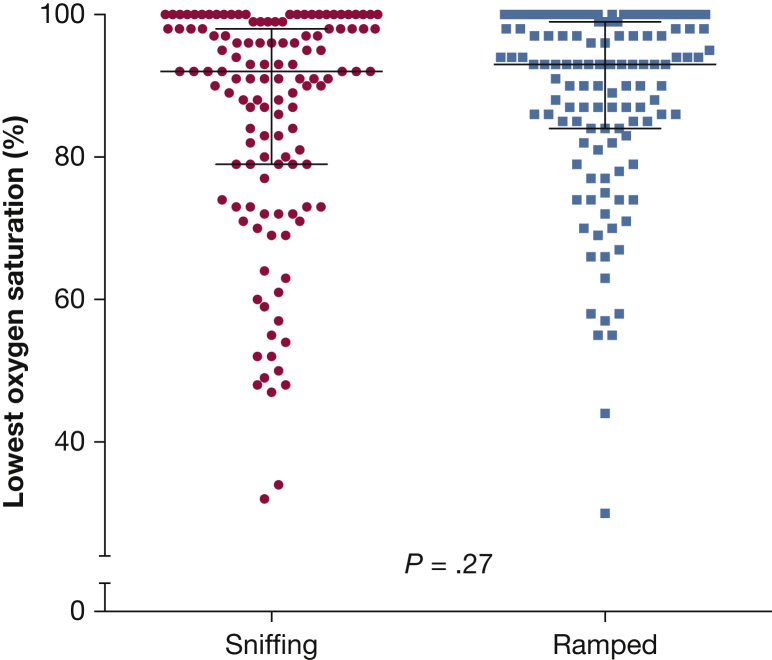
Methods: Multicenter, randomized trial comparing the ramped position (head of the bed elevated to 25°) with the sniffing position (torso supine, neck flexed, and head extended) among 260 adults undergoing endotracheal intubation by pulmonary and critical care medicine fellows in four ICUs between July 22, 2015, and July 19, 2016. The primary outcome was lowest arterial oxygen saturation between induction and 2 minutes after intubation. Secondary outcomes included Cormack-Lehane grade of glottic view, difficulty of intubation, and number of laryngoscopy attempts.
Results: The median lowest arterial oxygen saturation was 93% (interquartile range [IQR], 84%-99%) with the ramped position vs 92% (IQR, 79%-98%) with the sniffing position (P = .27). The ramped position appeared to increase the incidence of grade III or IV view (25.4% vs 11.5%, P = .01), increase the incidence of difficult intubation (12.3% vs 4.6%, P = .04), and decrease the rate of intubation on the first attempt (76.2% vs 85.4%, P = .02), respectively.
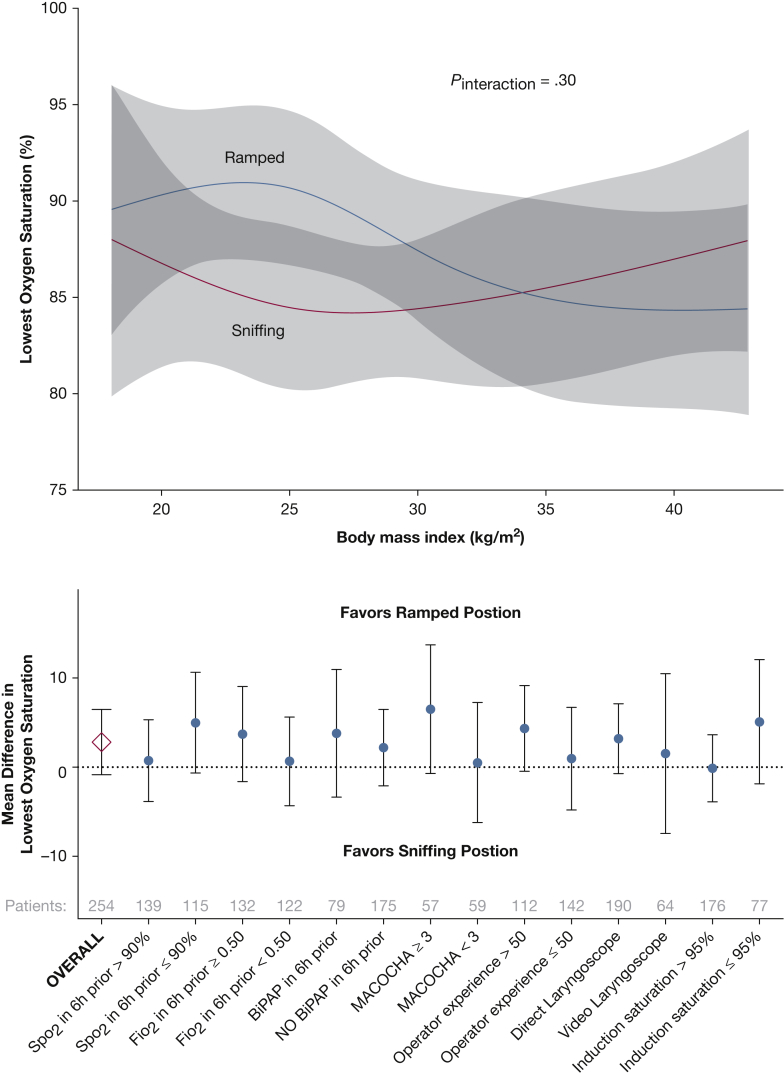
Conclusions: In this multicenter trial, the ramped position did not improve oxygenation during endotracheal intubation of critically ill adults compared with the sniffing position. The ramped position may worsen glottic view and increase the number of laryngoscopy attempts required for successful intubation.
Trial registry: ClinicalTrials.gov; No.: NCT02497729; URL: www.clinicaltrials.gov.
Keywords: endotracheal intubation; hypoxemia; randomized trial.
Copyright © 2017 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Should the Ramped Position Be "Sniffed at" in the ICU?Chest. 2017 Oct;152(4):693-694. doi: 10.1016/j.chest.2017.06.002. Chest. 2017. PMID: 28991539 No abstract available.
-
Comparing Ramped Position vs Sniffing Position for Intubation: Study Design Is Crucial.Chest. 2017 Nov;152(5):1091-1092. doi: 10.1016/j.chest.2017.07.018. Chest. 2017. PMID: 29126525 No abstract available.
-
Response.Chest. 2017 Nov;152(5):1092-1093. doi: 10.1016/j.chest.2017.07.017. Chest. 2017. PMID: 29126526 No abstract available.
-
Optimal Position for Intubation in the ICU: An Uneven Playing Field?Chest. 2017 Dec;152(6):1350. doi: 10.1016/j.chest.2017.09.034. Chest. 2017. PMID: 29223263 No abstract available.
-
Response.Chest. 2017 Dec;152(6):1351. doi: 10.1016/j.chest.2017.09.032. Chest. 2017. PMID: 29223265 Free PMC article. No abstract available.
-
Ramped Position: What the "Neck"!Chest. 2018 Feb;153(2):567-568. doi: 10.1016/j.chest.2017.09.054. Chest. 2018. PMID: 29406219 No abstract available.
-
Response.Chest. 2018 Feb;153(2):568-569. doi: 10.1016/j.chest.2017.11.022. Chest. 2018. PMID: 29406220 No abstract available.
References
-
- Baillard C., Fosse J.-P., Sebbane M. Noninvasive ventilation improves preoxygenation before intubation of hypoxic patients. Am J Respir Crit Care Med. 2006;174(2):171–177. - PubMed
-
- Mort T.C. The incidence and risk factors for cardiac arrest during emergency tracheal intubation: a justification for incorporating the ASA guidelines in the remote location. J Clin Anesth. 2004;16(7):508–516. - PubMed
-
- De Jong A., Molinari N., Terzi N. Early identification of patients at risk for difficult intubation in the intensive care unit: development and validation of the MACOCHA score in a multicenter cohort study. Am J Respir Crit Care Med. 2013;187(8):832–839. - PubMed
-
- Ibañez J., Raurich J.M. Normal values of functional residual capacity in the sitting and supine positions. Intensive Care Med. 1982;8(4):173–177. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
