

Safety of Rituximab Compared with Steroids and Cyclophosphamide for Idiopathic Membranous Nephropathy
- PMID: 28487395
- PMCID: PMC5576929
- DOI: 10.1681/ASN.2016091022
Safety of Rituximab Compared with Steroids and Cyclophosphamide for Idiopathic Membranous Nephropathy
Abstract
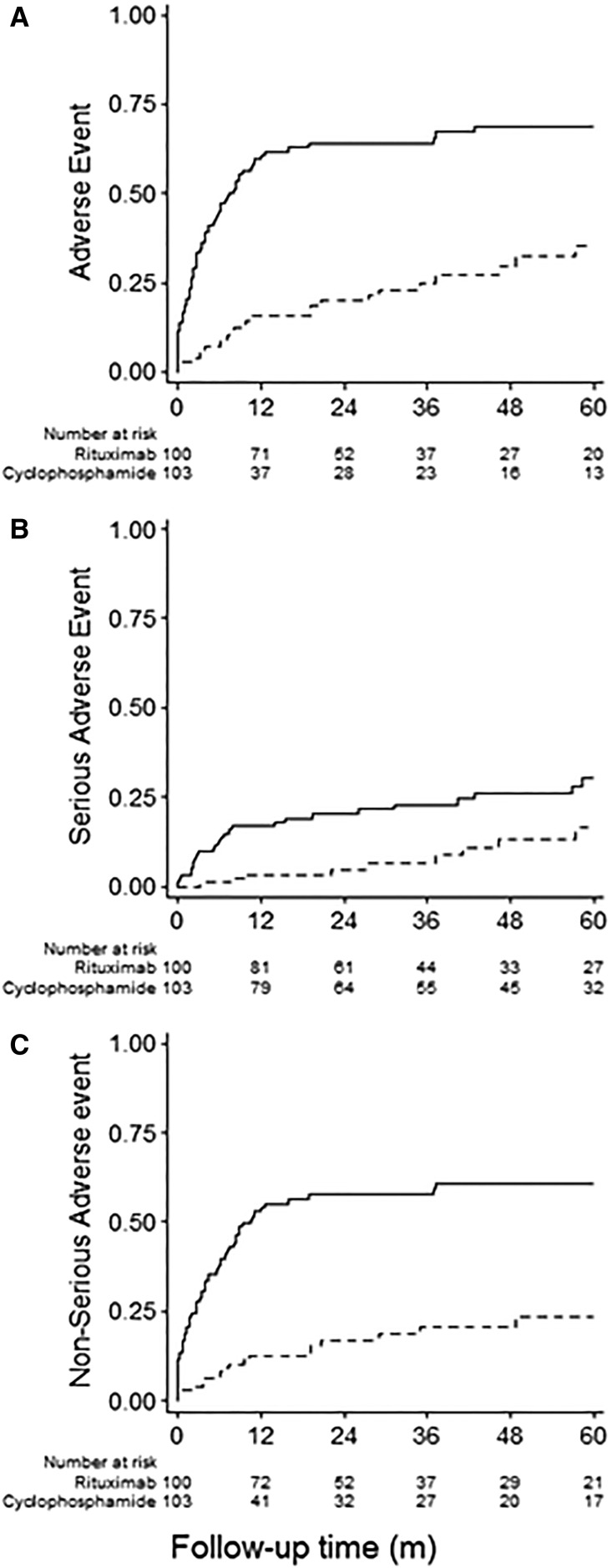
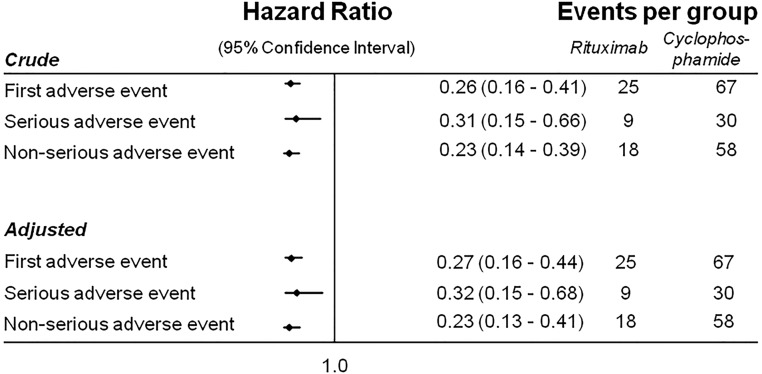
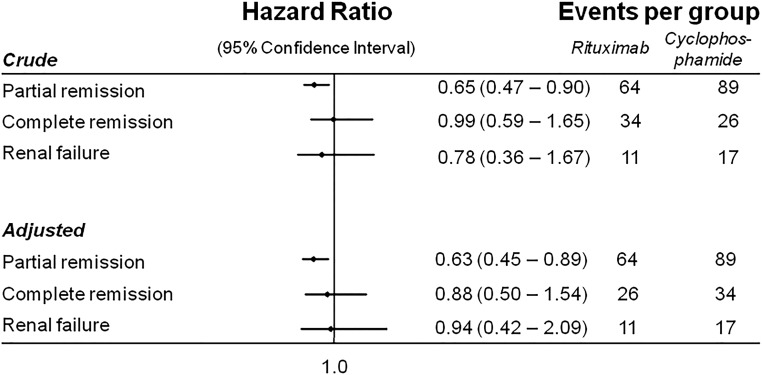
Guidelines recommend steroid plus cyclical cyclophosphamide (St-Cp) therapy for patients with idiopathic membranous nephropathy at high risk of progression to ESRD. Rituximab (Rtx) may be a safer alternative. In this retrospective, observational cohort study, we compared time to any adverse event (primary outcome); serious or nonserious events; partial and complete remission of the nephrotic syndrome; and a composite of doubling of serum creatinine, ESRD, or death between 100 Rtx-treated patients and 103 patients who received daily St-Cp We monitored patients with standardized protocols and adjusted for baseline characteristics by Cox regression. Over a median follow-up of 40 months, the Rtx group had significantly fewer adverse events than the St-Cp group (63 versus 173; P<0.001), both serious (11 versus 46; P<0.001) and nonserious (52 versus 127; P<0.001). Cumulative incidence of any first (35.5% versus 69.0%; P<0.001), serious (16.4% versus 30.2%; P=0.002), or nonserious (23.6% versus 60.8%; P<0.001) event was significantly lower with Rtx Adjusted hazard ratios (95% confidence intervals) between Rtx and St-Cp groups were 0.27 (0.16 to 0.44) for any first adverse event, 0.32 (0.15 to 0.68) for serious adverse events, and 0.23 (0.13 to 0.41) for nonserious adverse events. Although the cumulative incidence of partial remission was lower in the Rtx group, rates of complete remission and the composite renal end point did not differ significantly between groups. Because of its superior safety profile, we suggest that Rtx might replace St-Cp as first-line immunosuppressive therapy in patients with idiopathic membranous nephropathy and nephrotic syndrome.
Keywords: adverse events; clinical epidemiology; cyclophosphamide; drug safety; membranous nephropathy; rituximab.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- KDIGO Glomerulonephritis Work Group: KDIGO clinical practice guideline for glomerulonephritis. Kidney Int Suppl 2: 186–197, 2012
-
- Ponticelli C, Zucchelli P, Passerini P, Cesana B, Locatelli F, Pasquali S, Sasdelli M, Redaelli B, Grassi C, Pozzi C: A 10-year follow-up of a randomized study with methylprednisolone and chlorambucil in membranous nephropathy. Kidney Int 48: 1600–1604, 1995 - PubMed
-
- Jha V, Ganguli A, Saha TK, Kohli HS, Sud K, Gupta KL, Joshi K, Sakhuja V: A randomized, controlled trial of steroids and cyclophosphamide in adults with nephrotic syndrome caused by idiopathic membranous nephropathy. J Am Soc Nephrol 18: 1899–1904, 2007 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
