

Geriatric Assessment Predicts Survival and Competing Mortality in Elderly Patients with Early Colorectal Cancer: Can It Help in Adjuvant Therapy Decision-Making?
- PMID: 28487465
- PMCID: PMC5553962
- DOI: 10.1634/theoncologist.2016-0462
Geriatric Assessment Predicts Survival and Competing Mortality in Elderly Patients with Early Colorectal Cancer: Can It Help in Adjuvant Therapy Decision-Making?
Abstract
Background: The challenge when selecting elderly patients with colorectal cancer (CRC) for adjuvant therapy is to estimate the likelihood that death from other causes will preclude cancer events from occurring. The aim of this paper is to evaluate whether comprehensive geriatric assessment (CGA) can predict survival and cancer-specific mortality in elderly CRC patients candidates for adjuvant therapy.
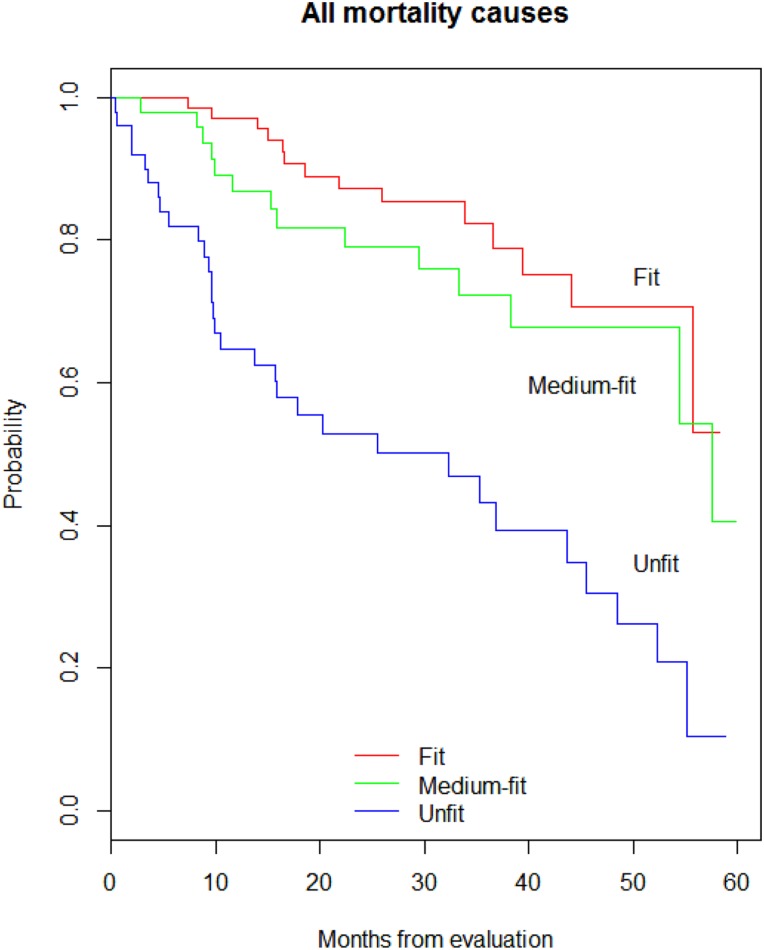
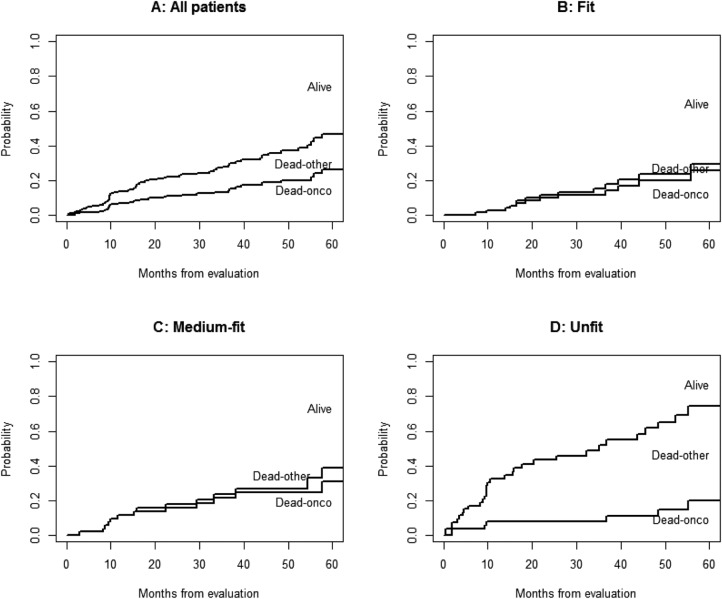
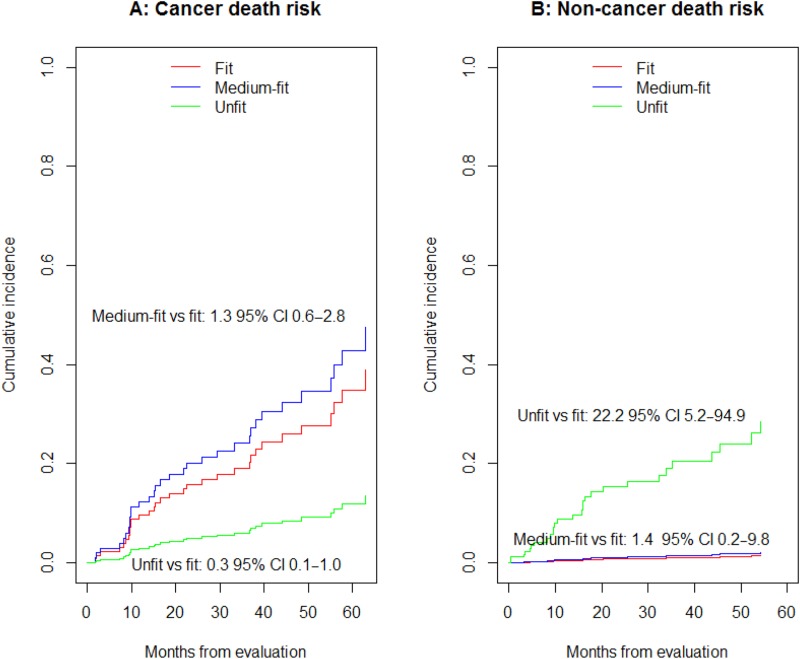
Material and methods: One hundred ninety-five consecutive patients aged ≥75 with high-risk stage II and stage III CRC were prospectively included from May 2008 to May 2015. All patients underwent CGA, which evaluated comorbidity, polypharmacy, functional status, geriatric syndromes, mood, cognition, and social support. According to CGA results, patients were classified into three groups-fit, medium-fit, and unfit-to receive standard therapy, adjusted treatment, and best supportive care, respectively. We recorded survival and cause of death and used the Fine-Gray regression model to analyze competing causes of death.
Results: Following CGA, 85 (43%) participants were classified as fit, 57 (29%) as medium-fit, and 53 (28%) as unfit. The univariate 5-year survival rates were 74%, 52%, and 27%. Sixty-one (31%) patients died due to cancer progression (53%), non-cancer-related cause (46%), and unknown reasons (1%); there were no toxicity-related deaths. Fit and medium-fit participants were more likely to die due to cancer progression, whereas patients classified as unfit were at significantly greater risk of non-cancer-related death.
Conclusion: CGA showed efficacy in predicting survival and discriminating between causes of death in elderly patients with high-risk stage II and stage III resected CRC, with potential implications for shaping the decision-making process for adjuvant therapies.
Implications for practice: Adjuvant therapy in elderly patients with colorectal cancer is controversial due to the high risk for competing events among these patients. In order to effectively select older patients for adjuvant therapy, we have to weigh the risk of cancer-related mortality and the potential survival benefits with treatment against the patient's life expectancy, irrespective of cancer. This prospective study focused on the prognostic value of geriatric assessment for survival using a competing-risk analysis approach, providing an important contribution on the treatment decision-making process and helping clinicians to identify elderly patients who might benefit from adjuvant chemotherapy among those who will not.
Keywords: Adjuvant therapy; Colorectal cancer; Competing risk model; Comprehensive geriatric assessment; Decision‐making; Elderly.
© AlphaMed Press 2017.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Shih YC, Hurria A. Preparing for an epidemic: Cancer care in an aging population. Am Soc Clin Oncol Educ Book 2014:133–137. - PubMed
-
- Siegel R, Ma J, Zou Z et al. Cancer statistics, 2014. CA Cancer J Clin 2014;64:9–29. - PubMed
-
- National Cancer Institute: Surveillance, Epidemiology, and End Results Program: SEER Fact Sheets‐Colon and rectum Cancer. Available at https://seer.cancer.gov/statfacts/html/colorect.html. Accessed April 4, 2017.
-
- Brenner H, Bouvier AM, Foschi R et al. Progress in colorectal cancer survival in Europe from the late 1980s to the early 21st century: The EUROCARE study. Int J Cancer 2012;131:1649–1658. - PubMed
-
- Holleczek B, Rossi S, Domenic A et al. On‐going improvement and persistent differences in the survival for patients with colon and rectum cancer across Europe 1999–2007—Results from the EUROCARE‐5 study. Eur J Cancer 2015. [Epub ahead of print]. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
