

Optimal treatment for Siewert type II and III adenocarcinoma of the esophagogastric junction: A retrospective cohort study with long-term follow-up
- PMID: 28487609
- PMCID: PMC5403751
- DOI: 10.3748/wjg.v23.i15.2723
Optimal treatment for Siewert type II and III adenocarcinoma of the esophagogastric junction: A retrospective cohort study with long-term follow-up
Abstract
Aim: To determine the optimal treatment strategy for Siewert type II and III adenocarcinoma of the esophagogastric junction.
Methods: We retrospectively reviewed the medical records of 83 patients with Siewert type II and III adenocarcinoma of the esophagogastric junction and calculated both an index of estimated benefit from lymph node dissection for each lymph node (LN) station and a lymph node ratio (LNR: ratio of number of positive lymph nodes to the total number of dissected lymph nodes). We used Cox proportional hazard models to clarify independent poor prognostic factors. The median duration of observation was 73 mo.
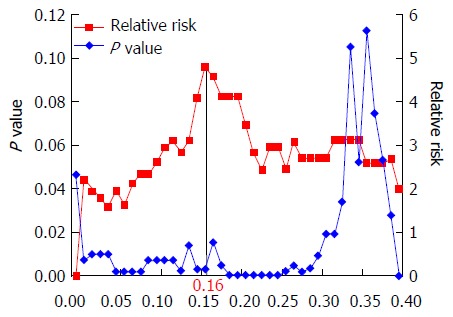
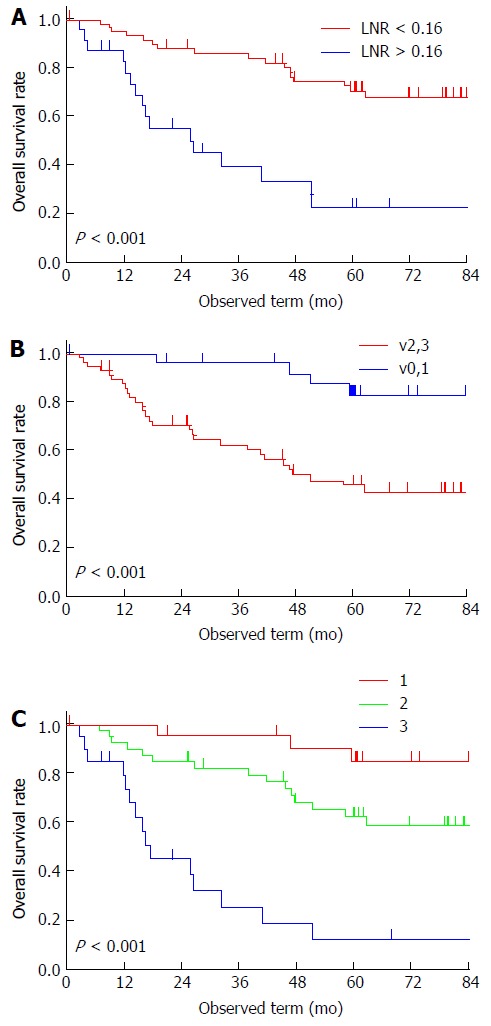
Results: Indices of estimated benefit from LN dissection were as follows, in descending order: lymph nodes (LN) along the lesser curvature, 26.5; right paracardial LN, 22.8; left paracardial LN, 11.6; LN along the left gastric artery, 10.6. The 5-year overall survival (OS) rate was 58%. Cox regression analysis revealed that vigorous venous invasion (v2, v3) (HR = 5.99; 95%CI: 1.71-24.90) and LNR of > 0.16 (HR = 4.29, 95%CI: 1.79-10.89) were independent poor prognostic factors for OS.
Conclusion: LN along the lesser curvature, right and left paracardial LN, and LN along the left gastric artery should be dissected in patients with Siewert type II or III adenocarcinoma of the esophagogastric junction. Patients with vigorous venous invasion and LNR of > 0.16 should be treated with aggressive adjuvant chemotherapy to improve survival outcomes.
Keywords: Adenocarcinoma of the esophagogastric junction; Lymph node dissection; Lymph node ratio; Prognostic factor; Venous invasion.
Conflict of interest statement
Conflict-of-interest statement: No potential conflicts of interest relevant to this article were reported.
Figures
References
-
- Devesa SS, Blot WJ, Fraumeni JF. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer. 1998;83:2049–2053. - PubMed
-
- Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97:142–146. - PubMed
-
- Kusano C, Gotoda T, Khor CJ, Katai H, Kato H, Taniguchi H, Shimoda T. Changing trends in the proportion of adenocarcinoma of the esophagogastric junction in a large tertiary referral center in Japan. J Gastroenterol Hepatol. 2008;23:1662–1665. - PubMed
-
- Blaser MJ, Saito D. Trends in reported adenocarcinomas of the oesophagus and gastric cardia in Japan. Eur J Gastroenterol Hepatol. 2002;14:107–113. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
