

Age-related impairment of esophagogastric junction relaxation and bolus flow time
- PMID: 28487616
- PMCID: PMC5403758
- DOI: 10.3748/wjg.v23.i15.2785
Age-related impairment of esophagogastric junction relaxation and bolus flow time
Abstract
Aim: To investigate the functional effects of abnormal esophagogastric (EGJ) measurements in asymptomatic healthy volunteers over eighty years of age.
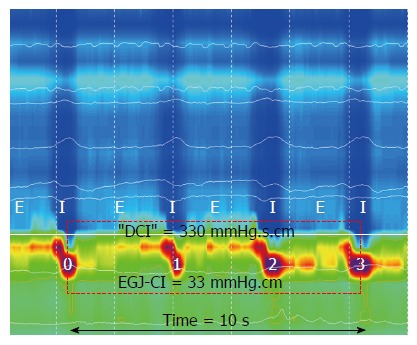
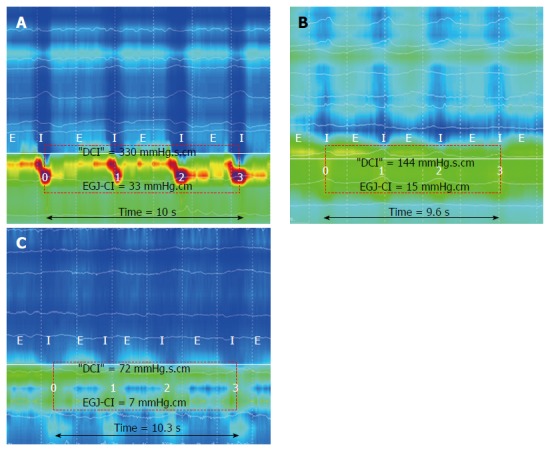
Methods: Data from 30 young controls (11 M, mean age 37 ± 11 years) and 15 aged subjects (9 M, 85 ± 4 years) were compared for novel metrics of EGJ-function: EGJ-contractile integral (EGJ-CI), "total" EGJ-CI and bolus flow time (BFT). Data were acquired using a 3.2 mm, 25 pressure (1 cm spacing) and 12 impedance segment (2 cm) solid-state catheter (Unisensor and MMS Solar GI system) across the EGJ. Five swallows each of 5 mL liquid (L) and viscous (V) bolus were analyzed. Mean values were compared using Student's t test for normally distributed data or Mann Whitney U-test when non-normally distributed. A P value < 0.05 was considered significant.
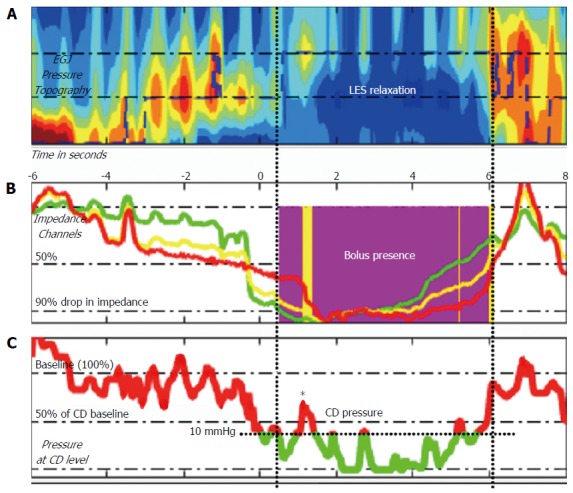
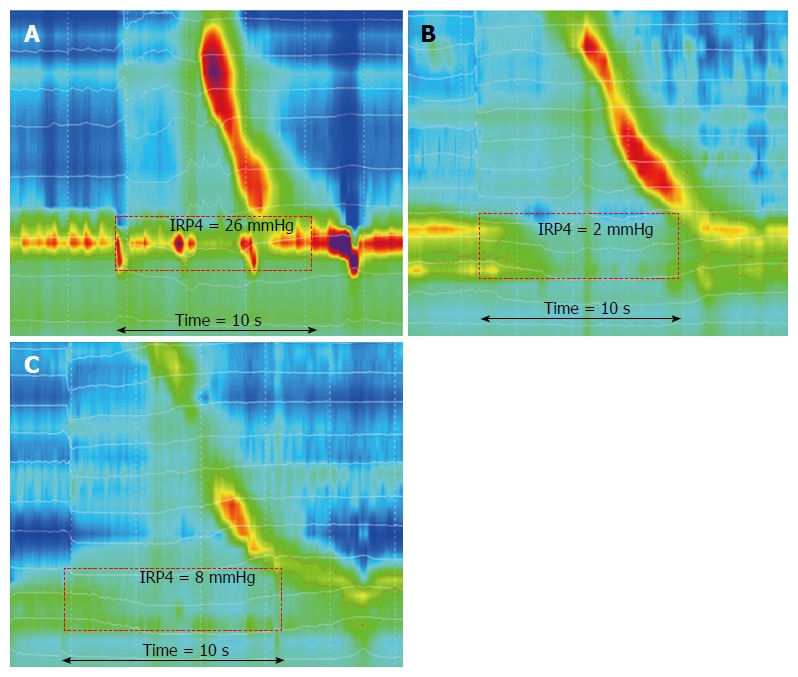
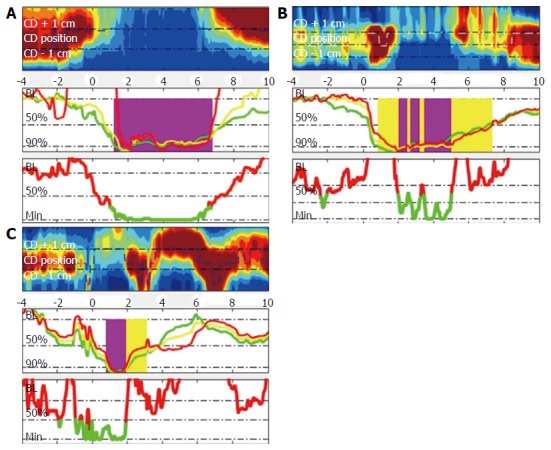
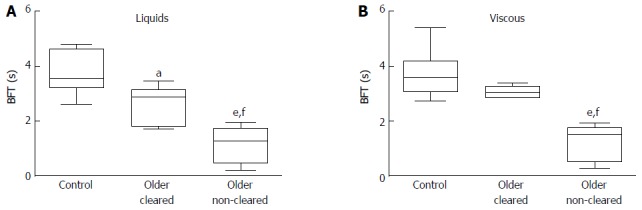
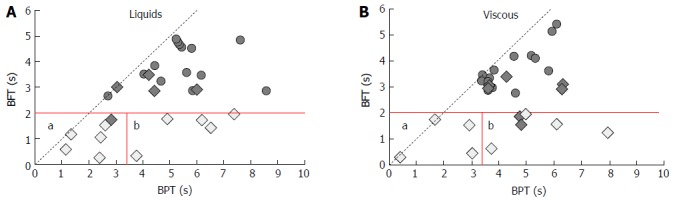
Results: EGJ-CI at rest was similar for older subjects compared to controls. "Total" EGJ-CI, measured during liquid swallowing, was increased in older individuals when compared to young controls (O 39 ± 7 mmHg.cm vs C 18 ± 3 mmHg.cm; P = 0.006). For both liquid and viscous bolus consistencies, IRP4 was increased (L: 11.9 ± 2.3 mmHg vs 5.9 ± 1.0 mmHg, P = 0.019 and V: 14.3 ± 2.4 mmHg vs 7.3 ± 0.8 mmHg; P = 0.02) and BFT was reduced (L: 1.7 ± 0.3 s vs 3.8 ± 0.2 s and V: 1.9 ± 0.3 s vs 3.8 ± 0.2 s; P < 0.001 for both) in older subjects, when compared to young. A matrix of bolus flow and presence above the EGJ indicated reductions in bolus flow at the EGJ occurred due to both impaired bolus transport through the esophageal body (i.e., the bolus never reached the EGJ) and increased flow resistance at the EGJ (i.e., the bolus retained just above the EGJ).
Conclusion: Bolus flow through the EGJ is reduced in asymptomatic older individuals. Both ineffective esophageal bolus transport and increased EGJ resistance contribute to impaired bolus flow.
Keywords: Aging; Esophagogastric junction; Esophagus; Impedance; Manometry; Pressure.
Conflict of interest statement
Conflict-of-interest statement: There are no conflicts of interest. Professor Omari owns a patent on AIM pressure flow analysis methods, which are not reported on for this study.
Figures
References
-
- Mittal RK, Goyal RK. Sphincter mechanisms at the lower end of the esophagus. GI Motility online. 2006
-
- Mittal RK. Lower esophageal sphincter in Motor function of the Pharynx, Esophagus, and its sphincters. Morgan and Claypool Life Sciences. St Rafael, CA, 2011 - PubMed
-
- Hershcovici T, Mashimo H, Fass R. The lower esophageal sphincter. Neurogastroenterol Motil. 2011;23:819–830. - PubMed
-
- Murray J, Du C, Ledlow A, Bates JN, Conklin JL. Nitric oxide: mediator of nonadrenergic noncholinergic responses of opossum esophageal muscle. Am J Physiol. 1991;261:G401–G406. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
