

Forearm Flexor Muscles in Children with Cerebral Palsy Are Weak, Thin and Stiff
- PMID: 28487645
- PMCID: PMC5403928
- DOI: 10.3389/fncom.2017.00030
Forearm Flexor Muscles in Children with Cerebral Palsy Are Weak, Thin and Stiff
Abstract
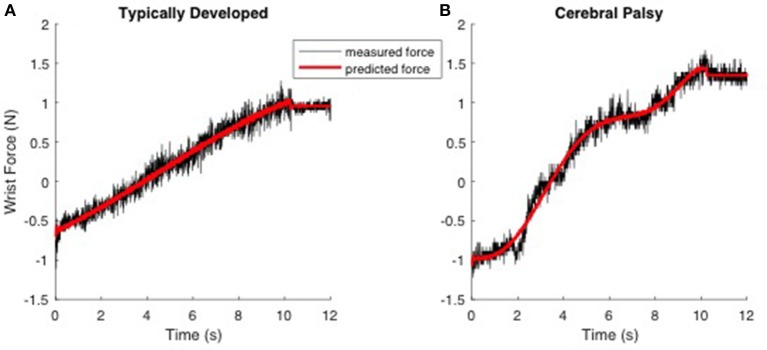
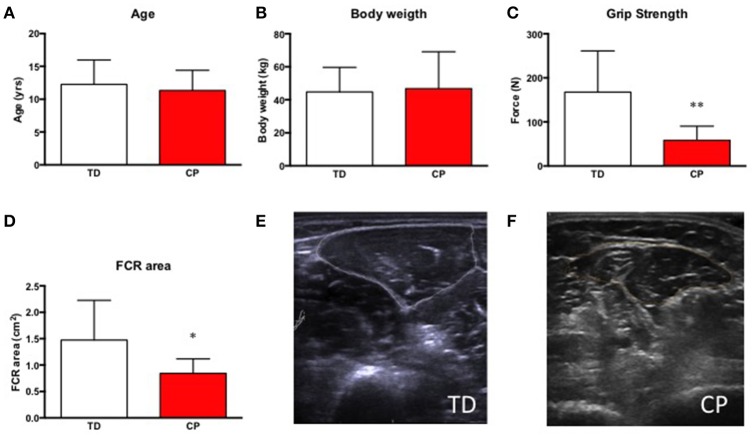
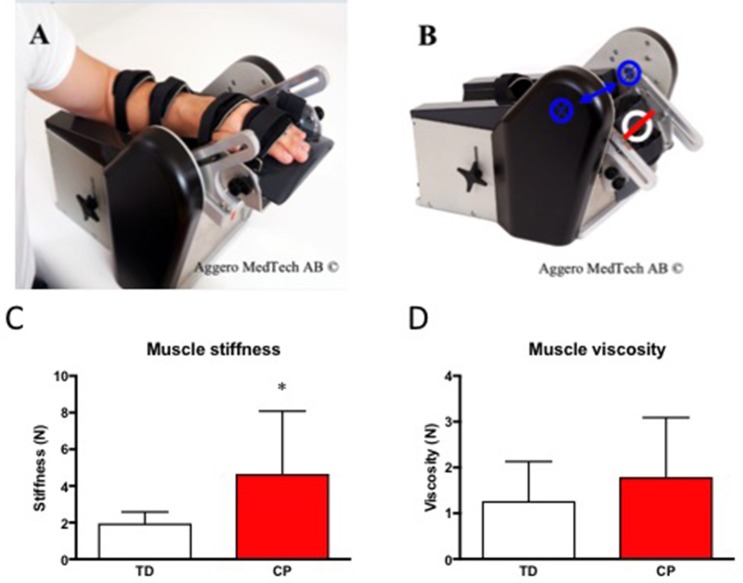
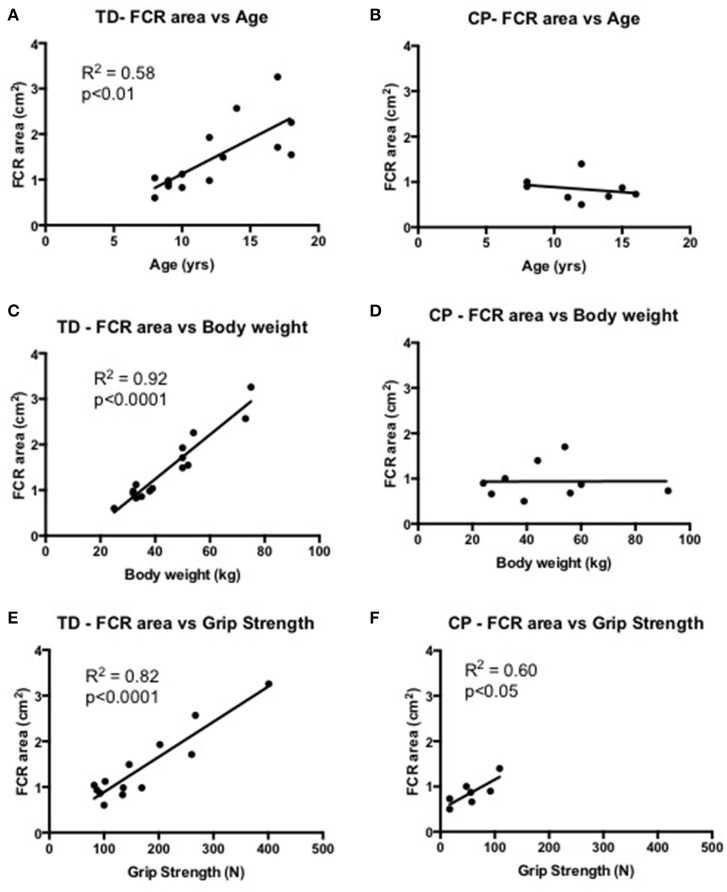
Children with cerebral palsy (CP) often develop reduced passive range of motion with age. The determining factor underlying this process is believed to be progressive development of contracture in skeletal muscle that likely changes the biomechanics of the joints. Consequently, to identify the underlying mechanisms, we modeled the mechanical characteristics of the forearm flexors acting across the wrist joint. We investigated skeletal muscle strength (Grippit®) and passive stiffness and viscosity of the forearm flexors in 15 typically developing (TD) children (10 boys/5 girls, mean age 12 years, range 8-18 yrs) and nine children with CP Nine children (6 boys/3 girls, mean age 11 ± 3 years (yrs), range 7-15 yrs) using the NeuroFlexor® apparatus. The muscle stiffness we estimate and report is the instantaneous mechanical response of the tissue that is independent of reflex activity. Furthermore, we assessed cross-sectional area of the flexor carpi radialis (FCR) muscle using ultrasound. Age and body weight did not differ significantly between the two groups. Children with CP had a significantly weaker (-65%, p < 0.01) grip and had smaller cross-sectional area (-43%, p < 0.01) of the FCR muscle. Passive stiffness of the forearm muscles in children with CP was increased 2-fold (p < 0.05) whereas viscosity did not differ significantly between CP and TD children. FCR cross-sectional area correlated to age (R2 = 0.58, p < 0.01), body weight (R2 = 0.92, p < 0.0001) and grip strength (R2 = 0.82, p < 0.0001) in TD children but only to grip strength (R2 = 0.60, p < 0.05) in children with CP. We conclude that children with CP have weaker, thinner, and stiffer forearm flexors as compared to typically developing children.
Keywords: cerebral palsy; muscle size; muscle stiffness; skeletal muscle; upper limb.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous