

Clinical Challenges in the Diagnosis and Treatment of Temporal Bone Osteomyelitis
- PMID: 28487802
- PMCID: PMC5401737
- DOI: 10.1155/2017/4097973
Clinical Challenges in the Diagnosis and Treatment of Temporal Bone Osteomyelitis
Abstract
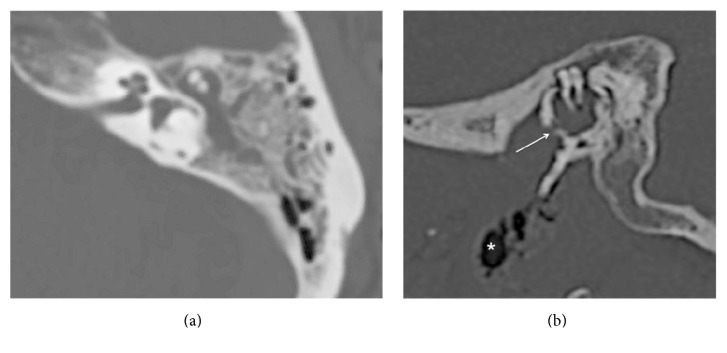
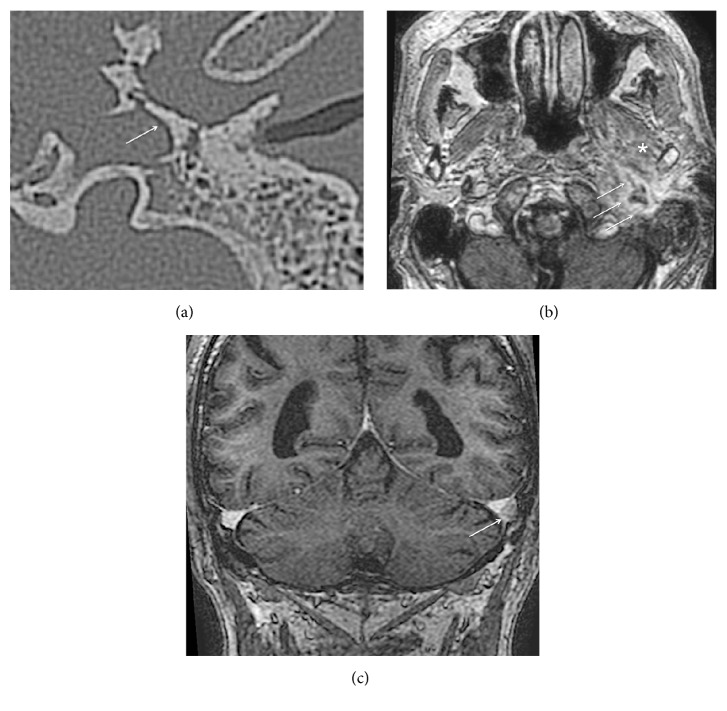
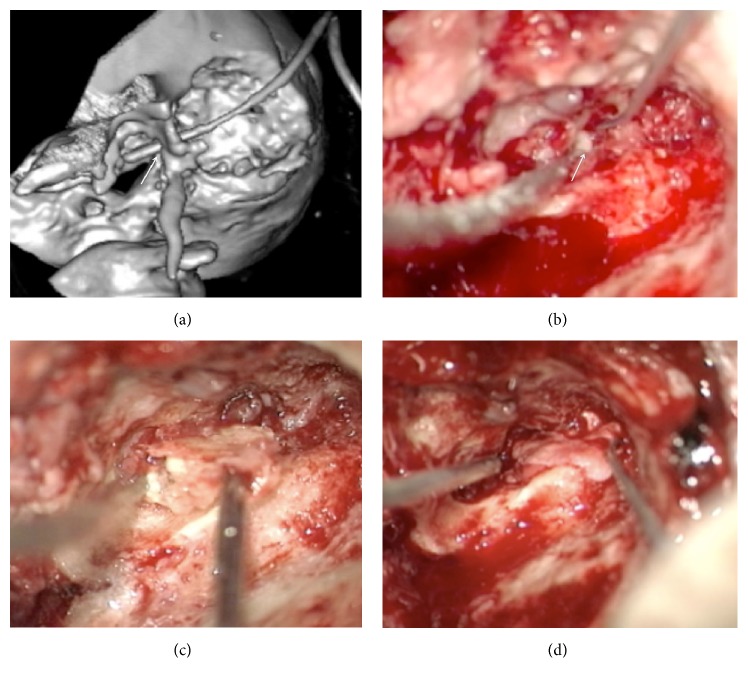
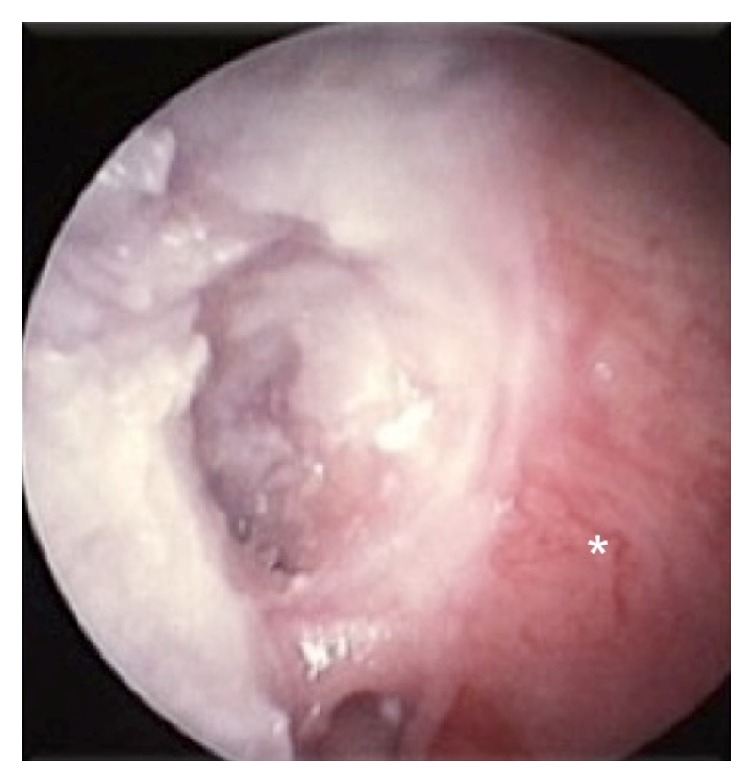
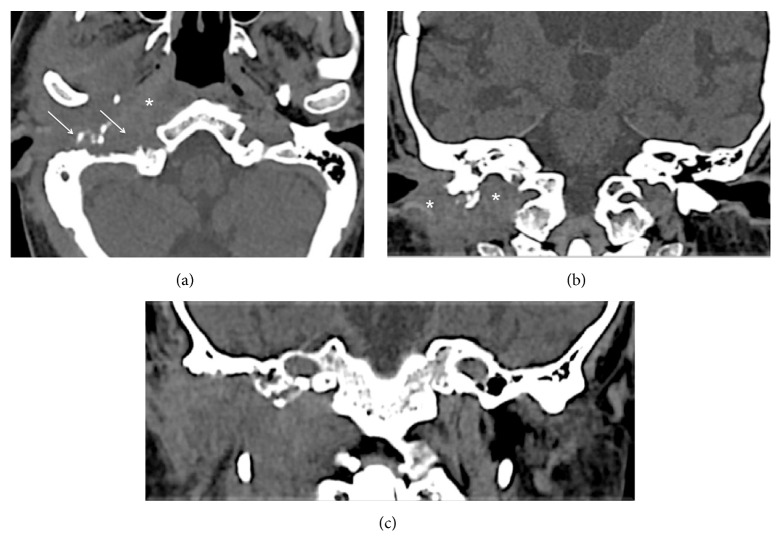
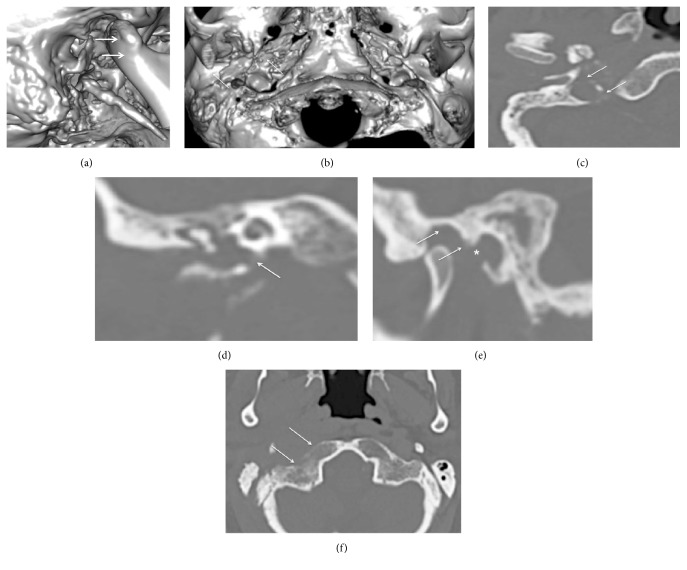
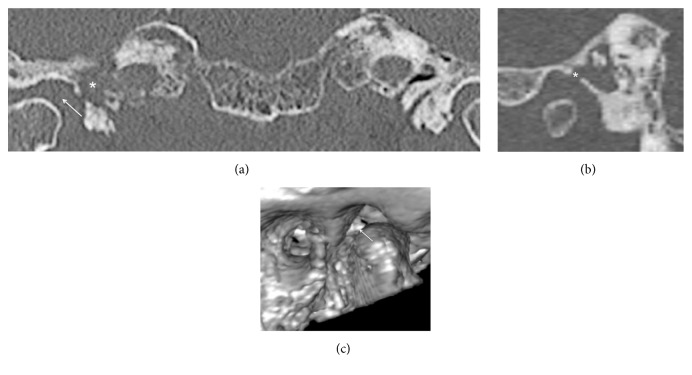
Temporal bone osteomyelitis is a serious life-threatening condition-a quick and proper diagnosis is needed to start treatment and reduce morbidity and mortality. Changing trends of the disease make a differential diagnosis difficult. To emphasize the importance of a clinical suspicion of this dangerous condition, our experience with three difficult cases is presented. The diagnosis was based on clinical symptoms, otoscopic findings, and findings on computed tomography or magnetic resonance imaging. Neoplasm and granulomatous inflammation were excluded by multiple biopsies. The disease can develop in nondiabetic patients. The disorder might be related to the initial inflammatory process in the middle ear with further direct spreading of infection through defects in the bony walls to deep temporal bone structures. Imaging should be performed early to detect osteolytic lesions of the skull base. Surgery was used for the presence of bone sequestra and infratemporal abscess.
Figures
References
-
- Slattery W. H., III, Brackmann D. E. Skull base osteomyelitis: malignant external otitis. Otolaryngologic Clinics of North America. 1996;29(5):795–806. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
