

LAPAROSCOPIC REPAIR OF LUMBAR HERNIA (GRYNFELT): TECHNICAL DESCRIPTION
- PMID: 28489172
- PMCID: PMC5424690
- DOI: 10.1590/0102-6720201700010016
LAPAROSCOPIC REPAIR OF LUMBAR HERNIA (GRYNFELT): TECHNICAL DESCRIPTION
Abstract
Background:: Lumbar hernias are rare. Usually manifest with reducible volume increase in the post-lateral region of the abdomen and may occur in two specific anatomic defects: the triangles of Grynfelt (upper) and Petit (lower). Despite controversies with better repair, laparoscopic approach, following the same principle of the treatment of inguinal hernias, seems to present significant advantages compared to conventional/open surgeries. However, some technical and anatomical details of the region, non usual to general surgeons, are fundamental for proper repair.
Aim:: To present systematization of laparoscopic transabdominal technique for repair of lumbar hernias with emphasis on anatomical details.
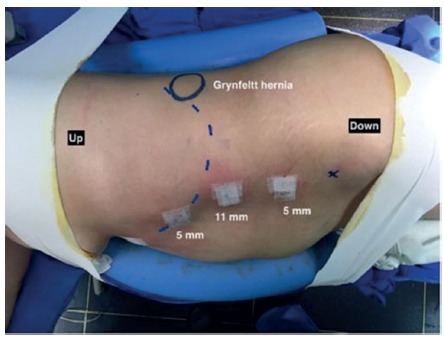
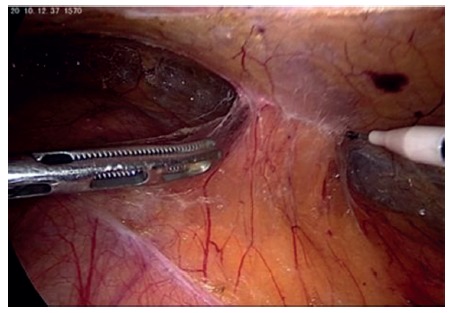
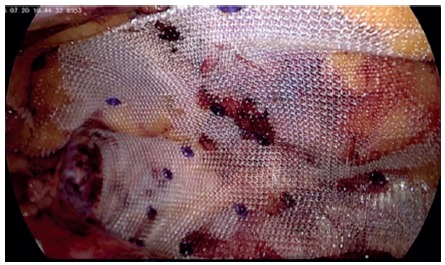
Method: : Patient is placed in the lateral decubitus. Laparoscopic access to abdominal cavity is performed by open technique on the left flank, 1.5 cm incision, followed by introduction of 11 mm trocar for a 30º scope. Two other 5 mm trocars, in the left anterior axillary line, are inserted into the abdominal cavity. The peritoneum of the left paracolic gutter is incised from the 10th rib to the iliac crest. Peritoneum and retroperitoneal is dissected. Reduction of all hernia contents is performed to demonstrate the hernia and its size. A 10x10 cm polypropylene mesh is introduced into the retroperitoneal space and fixed with absorbable staples covering the defect with at least 3-4 cm overlap. Subsequently, is carried out the closure of the peritoneum of paracolic gutter.
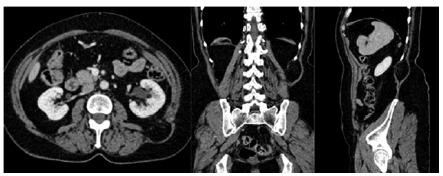
Results:: This technique was used in one patient with painful increased volume in the left lower back and bulging on the left lumbar region. CT scan was performed and revealed left superior lumbar hernia. Operative time was 45 min and there were no complications and hospitalization time of 24 h.
Conclusion:: As in inguinal hernia repair, laparoscopic approach is safe and effective for the repair of lumbar hernias, especially if the anatomical details are adequately respected.
Racional:: As hérnias lombares são raras. Geralmente se manifestam com aumento de volume redutível na região póstero-lateral do abdome e podem ocorrer em dois defeitos anatômicos específicos: os triângulos de Grynfelt (superior) e Petit (inferior). Apesar de controvérsias com relação a melhor forma de reparo, a abordagem laparoscópica, seguindo o mesmo princípio do tratamento das hérnias inguinais, parece apresentar vantagens significativas em relação às operações convencionais/abertas. Entretanto, alguns detalhes técnicos e anatômicos desta região, não usual aos cirurgiões gerais, são fundamentais para o adequado reparo.
Objetivo:: Apresentar sistematização da técnica laparoscópica transabdominal para a correção das hérnias lombares com ênfase nos detalhes anatômicos.
Método:: Paciente é colocado em decúbito lateral. O acesso laparoscópico à cavidade abdominal é realizado pela técnica aberta no flanco esquerdo, incisão de 1,5 cm, seguida pela introdução de trocárteres de 11 mm para ótica de 30º. Dois outros trocárteres de 5 mm, na linha axilar anterior esquerda, são inseridos na cavidade abdominal. O peritônio da goteira paracólica esquerda é incisado desde a 10ª costela até a crista ilíaca. O peritônio e o retroperitoneal são dissecados. A redução de todo o conteúdo de hérnia é realizada para demonstrar a hérnia e seu tamanho. Tela de polipropileno de 10x10 cm é introduzida no espaço retroperitoneal e fixada com grampos absorvíveis cobrindo o defeito com pelo menos 3-4 cm de sobreposição. Posteriormente, realiza-se o fechamento do peritônio da goteira paracólica.
Resultados:: Esta técnica foi utilizada em um paciente com aumento doloroso de volume na região lombar esquerda e abaulamento na região lombar esquerda. Tomografia computadorizada foi realizada e revelou hérnia lombar superior esquerda. O tempo operatório foi de 45 min e não houve complicações; o tempo de hospitalização de 24 h.
Conclusões:: Assim como no reparo das hérnias inguinais, a abordagem laparoscópica é segura e efetiva para as hérnias lombares, especialmente se os detalhes anatômicos forem adequadamente respeitados.
Racional:: As hérnias lombares são raras. Geralmente se manifestam com aumento de volume redutível na região póstero-lateral do abdome e podem ocorrer em dois defeitos anatômicos específicos: os triângulos de Grynfelt (superior) e Petit (inferior). Apesar de controvérsias com relação a melhor forma de reparo, a abordagem laparoscópica, seguindo o mesmo princípio do tratamento das hérnias inguinais, parece apresentar vantagens significativas em relação às operações convencionais/abertas. Entretanto, alguns detalhes técnicos e anatômicos desta região, não usual aos cirurgiões gerais, são fundamentais para o adequado reparo.
Objetivo:: Apresentar sistematização da técnica laparoscópica transabdominal para a correção das hérnias lombares com ênfase nos detalhes anatômicos.
Método:: Paciente é colocado em decúbito lateral. O acesso laparoscópico à cavidade abdominal é realizado pela técnica aberta no flanco esquerdo, incisão de 1,5 cm, seguida pela introdução de trocárteres de 11 mm para ótica de 30º. Dois outros trocárteres de 5 mm, na linha axilar anterior esquerda, são inseridos na cavidade abdominal. O peritônio da goteira paracólica esquerda é incisado desde a 10ª costela até a crista ilíaca. O peritônio e o retroperitoneal são dissecados. A redução de todo o conteúdo de hérnia é realizada para demonstrar a hérnia e seu tamanho. Tela de polipropileno de 10x10 cm é introduzida no espaço retroperitoneal e fixada com grampos absorvíveis cobrindo o defeito com pelo menos 3-4 cm de sobreposição. Posteriormente, realiza-se o fechamento do peritônio da goteira paracólica.
Resultados:: Esta técnica foi utilizada em um paciente com aumento doloroso de volume na região lombar esquerda e abaulamento na região lombar esquerda. Tomografia computadorizada foi realizada e revelou hérnia lombar superior esquerda. O tempo operatório foi de 45 min e não houve complicações; o tempo de hospitalização de 24 h.
Conclusões:: Assim como no reparo das hérnias inguinais, a abordagem laparoscópica é segura e efetiva para as hérnias lombares, especialmente se os detalhes anatômicos forem adequadamente respeitados.
Conflict of interest statement
Figures


Similar articles
-
Single transverse extended incision for radical neck dissection.Rev Col Bras Cir. 2016 Jul-Aug;43(4):270-5. doi: 10.1590/0100-69912016004012. Rev Col Bras Cir. 2016. PMID: 27679947 English, Portuguese.
-
Systematic training model for teaching, development and training of instructors in inguinal hernia treatment using the Lichtenstein technique. Hernia campaign 2014 & 2015.Rev Col Bras Cir. 2016 Sep-Oct;43(5):382-391. doi: 10.1590/0100-69912016005018. Rev Col Bras Cir. 2016. PMID: 27982333 English, Portuguese.
-
ANATOMIC VARIATIONS OF HEPATIC ARTERY: A STUDY IN 479 LIVER TRANSPLANTATIONS.Arq Bras Cir Dig. 2017 Jan-Mar;30(1):35-37. doi: 10.1590/0102-6720201700010010. Arq Bras Cir Dig. 2017. PMID: 28489166 Free PMC article.
-
Comparative study of abdominal cavity temporary closure techniques for damage control.Rev Col Bras Cir. 2016 Sep-Oct;43(5):368-373. doi: 10.1590/0100-69912016005015. Rev Col Bras Cir. 2016. PMID: 27982331 English, Portuguese.
-
O papel da estereorradiografia na avaliação das deformidades dos membros inferiores.Radiol Bras. 2022 Mar-Apr;55(2):104-112. doi: 10.1590/0100-3984.2021.0104. Radiol Bras. 2022. PMID: 35414732 Free PMC article. Review.
Cited by
-
Laparoscopic repair via the transabdominal preperitoneal procedure for bilateral lumbar hernia: Three cases report and review of literature.World J Clin Cases. 2018 Sep 26;6(10):398-405. doi: 10.12998/wjcc.v6.i10.398. World J Clin Cases. 2018. PMID: 30283803 Free PMC article.
-
A Case Report of Laparoscopic-Assisted Repair of a Rare Congenital Lumbar (Grynfeltt-Lesshaft) Hernia.Cureus. 2024 Nov 7;16(11):e73239. doi: 10.7759/cureus.73239. eCollection 2024 Nov. Cureus. 2024. PMID: 39651003 Free PMC article.
-
Sublay repair for primary superior lumbar hernia with the Kugel patch.ANZ J Surg. 2020 May;90(5):776-780. doi: 10.1111/ans.15866. Epub 2020 Mar 24. ANZ J Surg. 2020. PMID: 32207872 Free PMC article.
-
Single-incision retroperitoneal laparoscopic repair of superior lumbar hernia using self-fixating ProGrip mesh: A case report.Int J Surg Case Rep. 2020;67:120-122. doi: 10.1016/j.ijscr.2020.01.034. Epub 2020 Feb 6. Int J Surg Case Rep. 2020. PMID: 32062114 Free PMC article.
-
Endoscopic retroperitoneal repair of superior lumbar hernia (Grynfeltt hernia) using self-fixating mesh to prevent nerve injury: a case report.Surg Case Rep. 2024 Mar 5;10(1):52. doi: 10.1186/s40792-024-01846-5. Surg Case Rep. 2024. PMID: 38441792 Free PMC article.
References
-
- Barbette P. Lugduni. Vol. 26. Gelder: 1672. Opera chirurgico-anatomica.
-
- Cesar D, Valadão M, Murrahe RJ. Grynfelt hernia: case report and literature review. Hernia. 2012;16(1):107–111. - PubMed
-
- Loukas M, Tubbs R, El-Sedfy A, Jester A, Polepalli S, Kinsela C. The clinical anatomy of the triangle of petit. Hernia. 2007;11:441–444. - PubMed
-
- Loukas M, Tubbs RS, Shoja M. Lumbar hernia, anatomical basis and clinical aspects. Surg Radiol Anat. 2008;30:609–610. - PubMed
-
- Armstrong O, Hamel A, Grignon B. Lumbar hernia: Anatomical basis and clinical aspects. Surg Radiol Anat. 2008;30:533–537. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
