

Tai Chi Chih Compared With Cognitive Behavioral Therapy for the Treatment of Insomnia in Survivors of Breast Cancer: A Randomized, Partially Blinded, Noninferiority Trial
- PMID: 28489508
- PMCID: PMC5549450
- DOI: 10.1200/JCO.2016.71.0285
Tai Chi Chih Compared With Cognitive Behavioral Therapy for the Treatment of Insomnia in Survivors of Breast Cancer: A Randomized, Partially Blinded, Noninferiority Trial
Erratum in
-
Errata.J Clin Oncol. 2017 Dec 20;35(36):4096. doi: 10.1200/JCO.2017.76.9034. J Clin Oncol. 2017. PMID: 29244979 Free PMC article. No abstract available.
Abstract
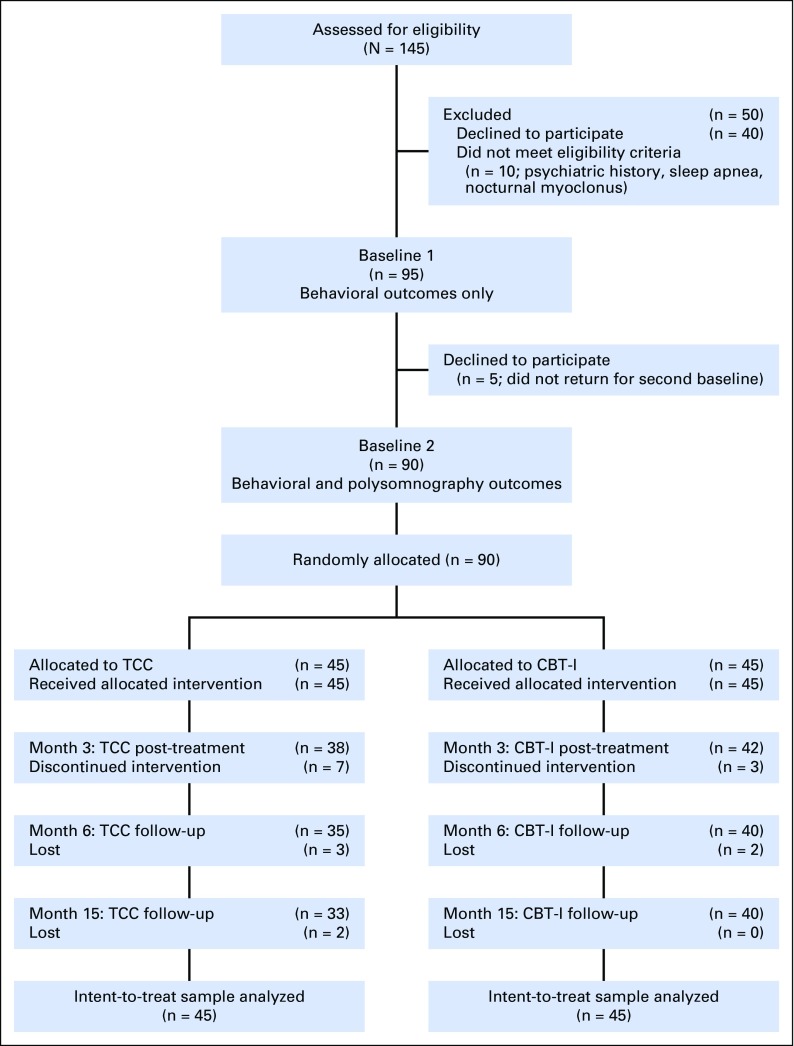
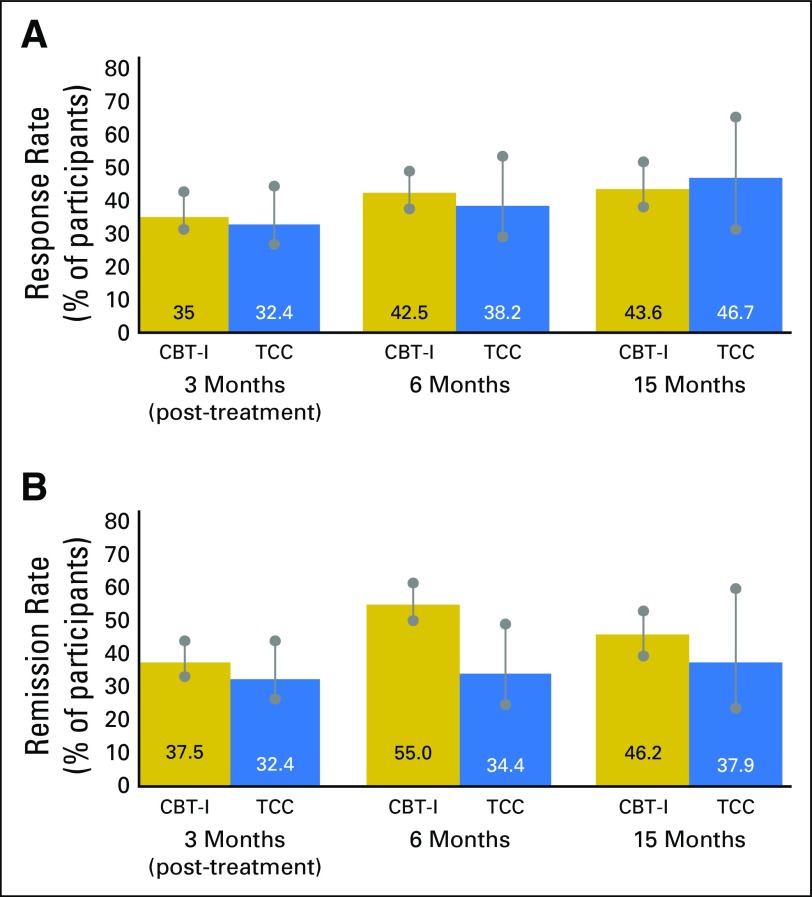
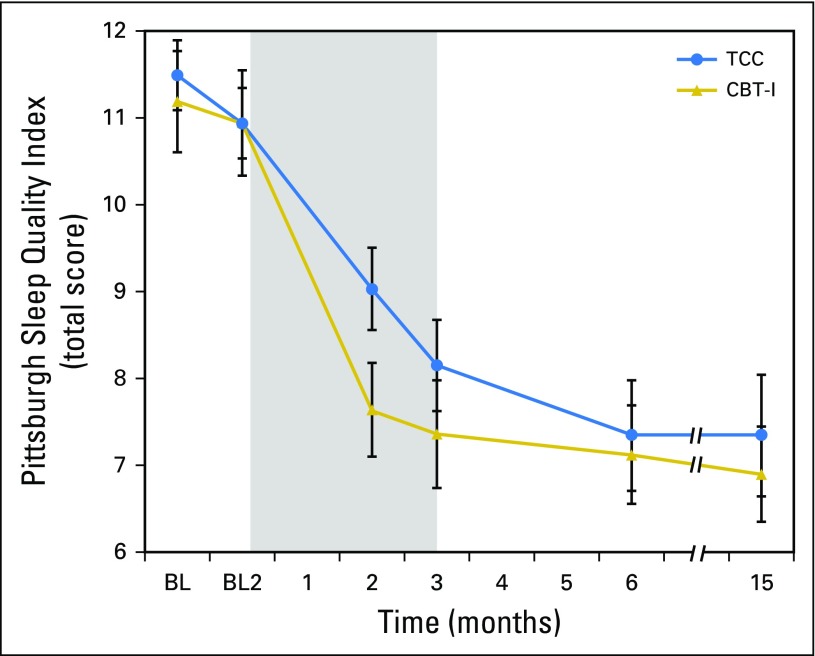
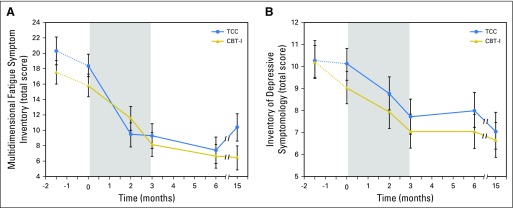
Purpose Cognitive behavioral therapy for insomnia (CBT-I) and Tai Chi Chih (TCC), a movement meditation, improve insomnia symptoms. Here, we evaluated whether TCC is noninferior to CBT-I for the treatment of insomnia in survivors of breast cancer. Patients and Methods This was a randomized, partially blinded, noninferiority trial that involved survivors of breast cancer with insomnia who were recruited from the Los Angeles community from April 2008 to July 2012. After a 2-month phase-in period with repeated baseline assessment, participants were randomly assigned to 3 months of CBT-I or TCC and evaluated at months 2, 3 (post-treatment), 6, and 15 (follow-up). Primary outcome was insomnia treatment response-that is, marked clinical improvement of symptoms by the Pittsburgh Sleep Quality Index-at 15 months. Secondary outcomes were clinician-assessed remission of insomnia; sleep quality; total sleep time, sleep onset latency, sleep efficiency, and awake after sleep onset, derived from sleep diaries; polysomnography; and symptoms of fatigue, sleepiness, and depression. Results Of 145 participants who were screened, 90 were randomly assigned (CBT-I: n = 45; TCC: n = 45). The proportion of participants who showed insomnia treatment response at 15 months was 43.7% and 46.7% in CBT-I and TCC, respectively. Tests of noninferiority showed that TCC was noninferior to CBT-I at 15 months ( P = .02) and at months 3 ( P = .02) and 6 ( P < .01). For secondary outcomes, insomnia remission was 46.2% and 37.9% in CBT-I and TCC, respectively. CBT-I and TCC groups showed robust improvements in sleep quality, sleep diary measures, and related symptoms (all P < .01), but not polysomnography, with similar improvements in both groups. Conclusion CBT-I and TCC produce clinically meaningful improvements in insomnia. TCC, a mindful movement meditation, was found to be statistically noninferior to CBT-I, the gold standard for behavioral treatment of insomnia.
Figures
References
-
- American Psychiatric Association . DSM-5 Task Force: Diagnostic and Statistical Manual of Mental Disorders. ed 5. Washington, DC: American Psychiatric Association; 2013.
-
- Savard J, Villa J, Ivers H, et al. Prevalence, natural course, and risk factors of insomnia comorbid with cancer over a 2-month period. J Clin Oncol. 2009;27:5233–5239. - PubMed
-
- Savard J, Ivers H, Villa J, et al. Natural course of insomnia comorbid with cancer: An 18-month longitudinal study. J Clin Oncol. 2011;29:3580–3586. - PubMed
-
- Ohayon MM. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med Rev. 2002;6:97–111. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
