

Comparison of local infiltration analgesia and sciatic nerve block as an adjunct to femoral nerve block for pain control after total knee arthroplasty: A systematic review and meta-analysis
- PMID: 28489762
- PMCID: PMC5428596
- DOI: 10.1097/MD.0000000000006829
Comparison of local infiltration analgesia and sciatic nerve block as an adjunct to femoral nerve block for pain control after total knee arthroplasty: A systematic review and meta-analysis
Abstract
Background: To perform a meta-analysis to assess the efficiency and safety between local infiltration analgesia (LIA) and sciatic nerve block (SNB) when combined with femoral nerve block (FNB) for pain control following total knee arthroplasty (TKA).
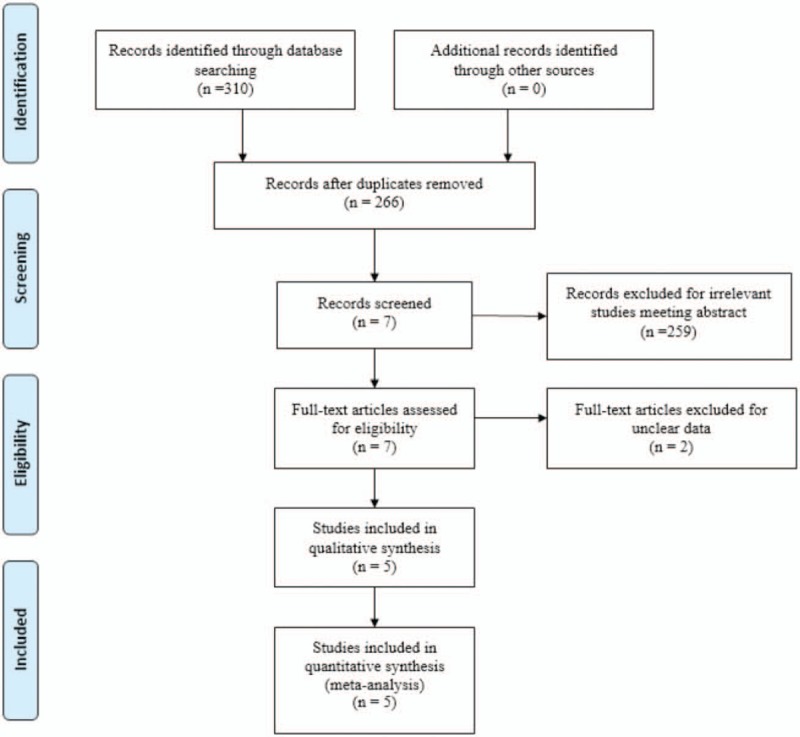
Methods: We systemically searched the following electronic databases for potentially relevant articles: Embase (1980-2017.01), Medline (1966-2017.01), PubMed (1966-2017.01), ScienceDirect (1985-2017.01), web of science (1950-2017.01) and the Cochrane Library. Only studies published in English that were accessible online were considered. Furthermore, we only considered studies that were published from 1966 to 2017. Only studies that met the following inclusion criteria were considered: (a) patients were adult human subjects who were set to undergo TKA; (b) the intervention was either SNB combined with FNB or LIA combined with FNB; (c) the outcomes of the studies, such as visual analog scale (VAS) scores, morphine consumption, length of stay and postoperative adverse effects, including the risk of nausea, vomiting and falls, were reported; (d) studies were either RCTs or non-RCT. Meta-analysis was performed using Stata 11.0 software. Modified Jadad score (7-points scale) which was based on Cochrane Handbook for Systematic Reviews of Interventions is used for assessment of RCTs. The Methodological Index for Nonrandomized Studies (MINORS) scale was used to assess non-RCTs with scores ranging 0 to 24. The synthesis of the outcomes for all studies was calculated as the weighted average rate by using a fixed or random effect model which depends on statistical heterogeneity. Systematic review registration number is CRD42017110661.
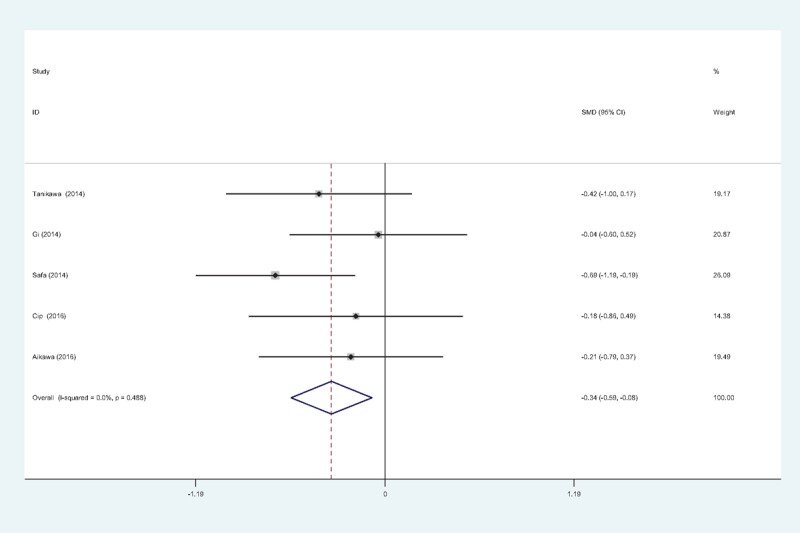
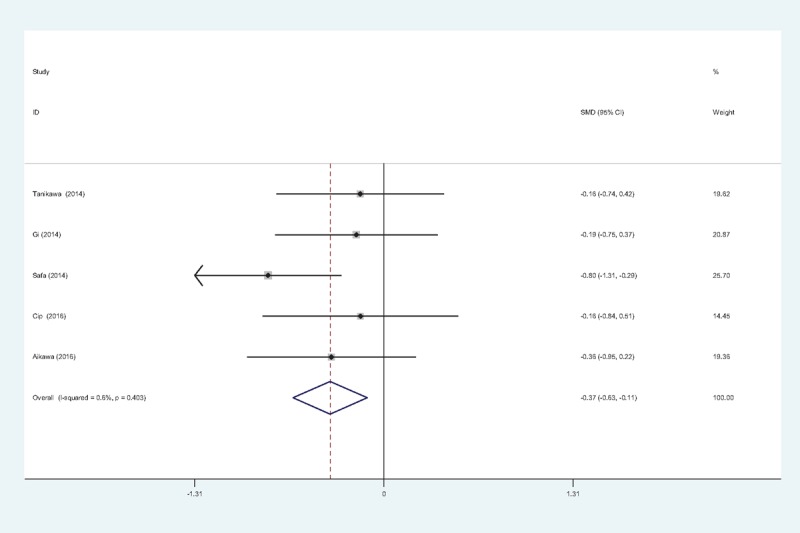
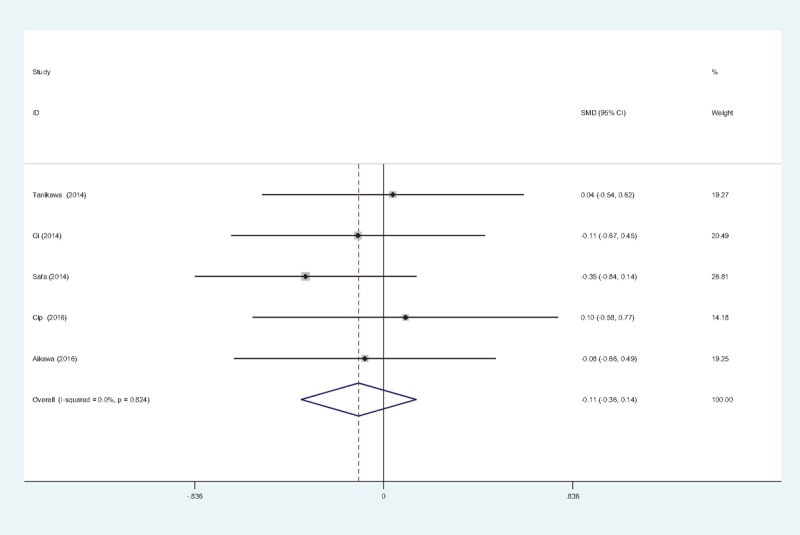
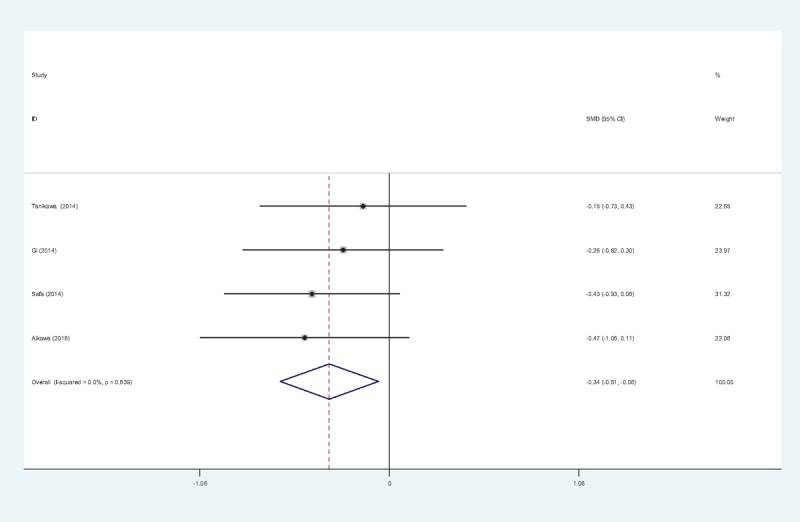
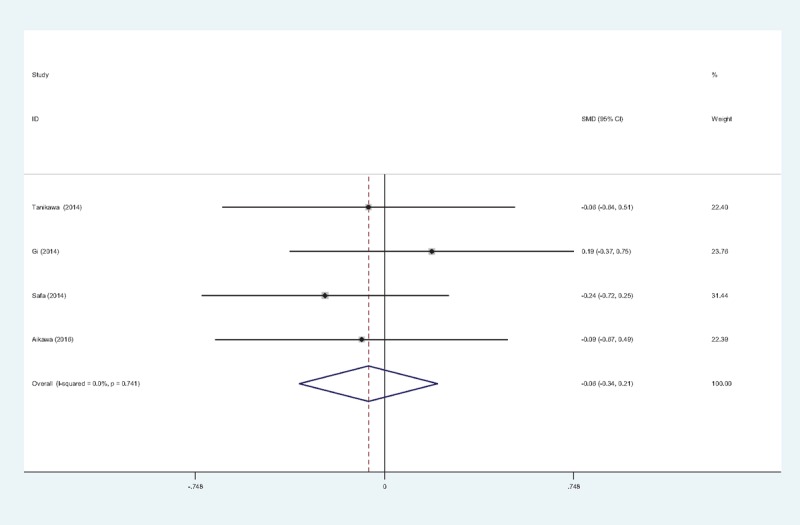
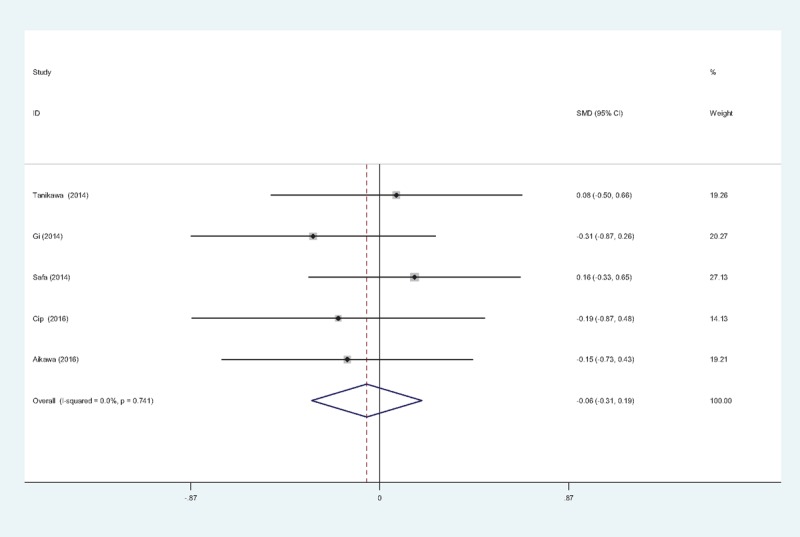
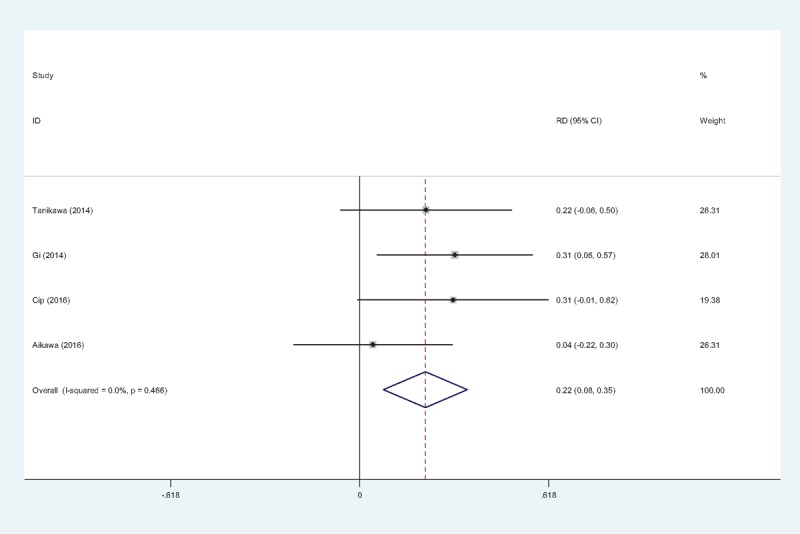
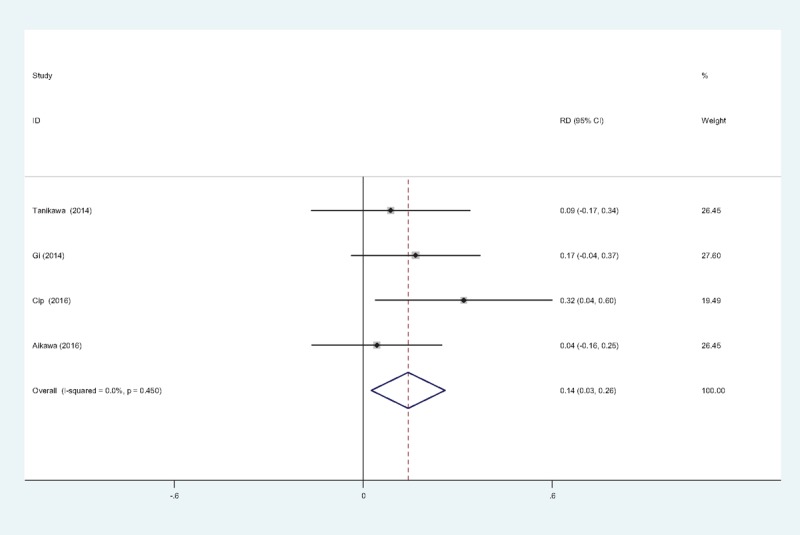
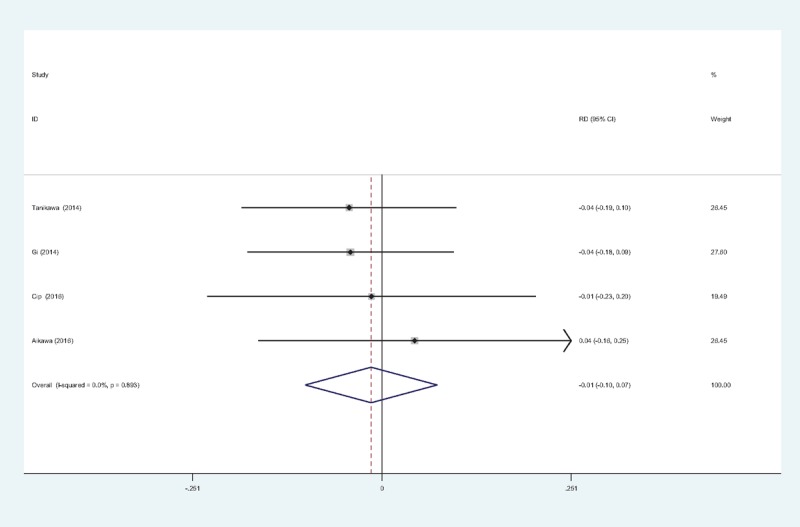
Results: Three randomized controlled trials (RCTs) and 2 nonrandomized controlled trials (Non-RCTs), including 240 patients met the inclusion criteria. The present meta-analysis indicated that there were significant differences between groups in terms of visual analog scale (VAS) score at 12 hours (SMD = -0.337, 95% CI: -0.593 to -0.081, P =.010), VAS score at 24 hours (SMD = -0.337, 95% CI: -0.612 to -0.061, P =.017), morphine equivalent consumption at 24 hours (SMD = -0.371, 95% CI: -0.627 to -0.114, P = .005) and incidence of nausea (RD = 0.215, 95% CI: 0.078 to 0.353, P = .002) and vomiting (RD = 0.143, 95% CI: 0.026 to 0.260, P = .017).
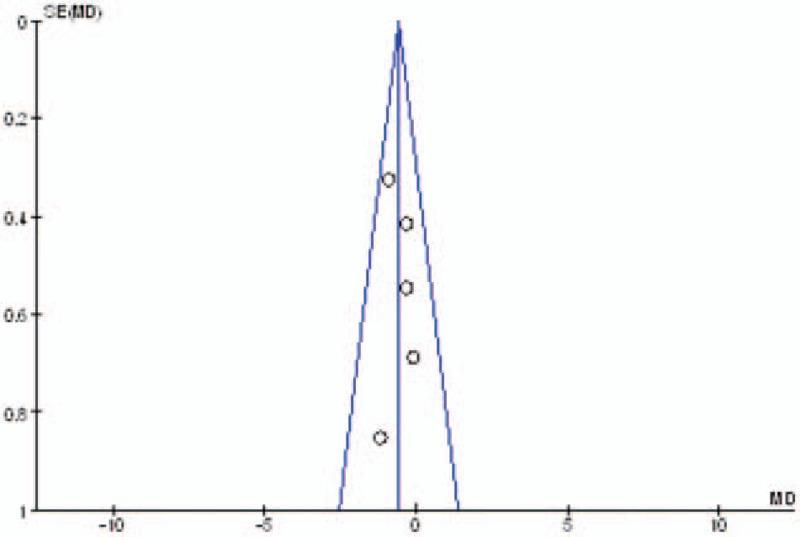
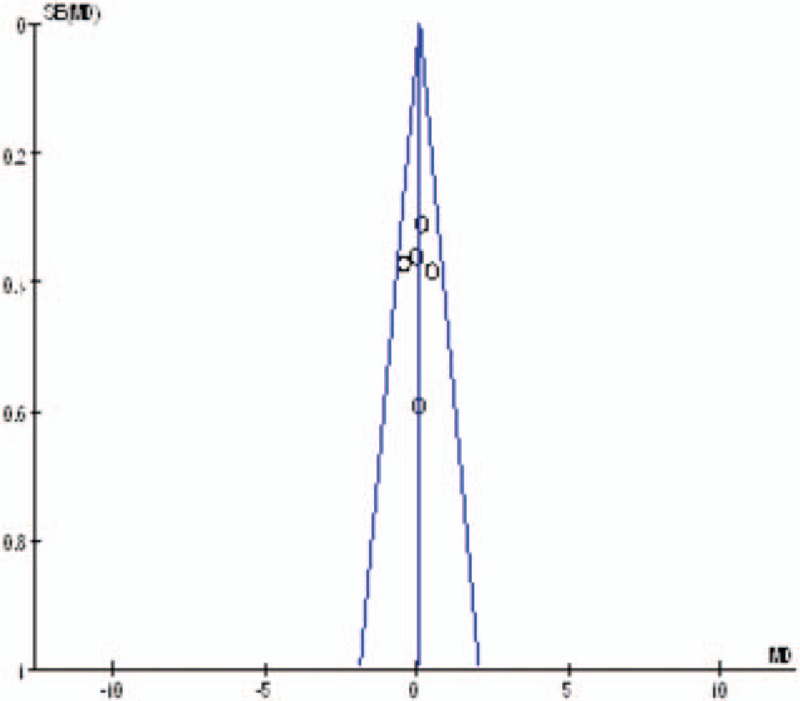
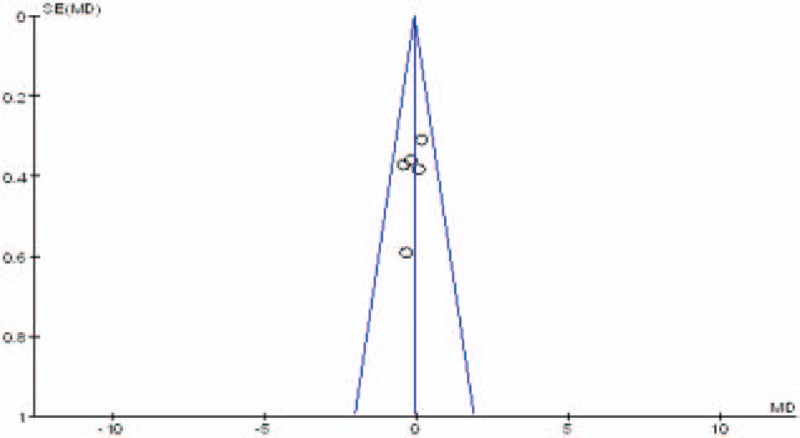
Conclusion: FNB combined with SNB provided decreased VAS scores and less morphine consumption at 12 and 24 hours compared with FNB combined with LIA in total knee arthroplasty. In addition, it was associated with lower risks of nausea and vomiting. We assessed the quality of the evidence as low to very low; therefore, our confidence in the effect estimate is limited, and the true effect may be substantially different from our estimates. Further studies should focus on surgeries that are known to be associated with significant postoperative pain, particularly surgeries where improved pain control may deliver significant clinical benefits through reduced morbidity, or cost-effectiveness benefits through faster rehabilitation and discharge. The present meta-analysis has the following limitations: (1) only 5 studies were included in the meta-analysis. Although all of them are recently published studies, the sample sizes are relatively small; (2) Functional outcome is an important parameter; however, owing to the insufficiency of relevant data, we failed to perform a meta-analysis on functional outcome; (3) The doses of anesthetics and the concomitant pain management regimes varied between the studies, which may have influenced the results; (4) The duration of follow-up was relatively short, which might have led to an underestimating of complications; and (5) publication bias present in the meta-analysis may have influenced the results.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Singelyn FJ, Deyaert M, Joris D, et al. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous three-in-one block on postoperative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg 1998;87:88–92. - PubMed
-
- Tripuraneni KR, Woolson ST, Giori NJ. Local infiltration analgesia in TKA patients reduces length of stay and postoperative pain scores. Orthopedics 2011;34:173. - PubMed
-
- Mullaji A, Kanna R, Shetty GM, et al. Efficacy of periarticular injection of bupivacaine, fentanyl, and methylprednisolone in total knee arthroplasty:a prospective, randomized trial. J Arthroplasty 2010;25:851–7. - PubMed
-
- Duellman TJ, Gaffigan C, Milbrandt JC, et al. Multi-modal, pre-emptive analgesia decreases the length of hospital stay following total joint arthroplasty. Orthopedics 2009;32:167. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
