

Chronic active Epstein-Barr virus infection associated with hemophagocytic syndrome and extra-nodal natural killer/T-cell lymphoma in an 18-year-old girl: A case report
- PMID: 28489771
- PMCID: PMC5428605
- DOI: 10.1097/MD.0000000000006845
Chronic active Epstein-Barr virus infection associated with hemophagocytic syndrome and extra-nodal natural killer/T-cell lymphoma in an 18-year-old girl: A case report
Abstract
Rationale: Chronic active Epstein-Barr virus infection (CAEBV) associated with hemophagocytic syndrome (HPS) and extra-nodal natural killer (NK)/T-cell lymphoma (ENKL) is a rare life-threatening disorder. This disease is easily misdiagnosed because of its varied presentations.
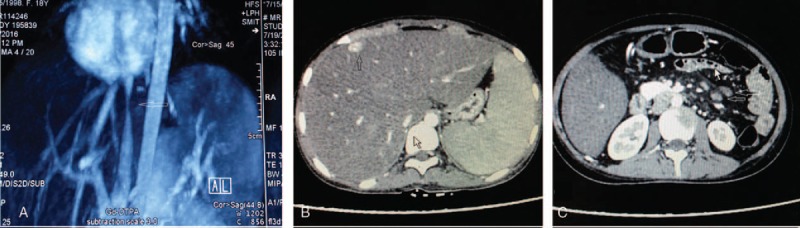
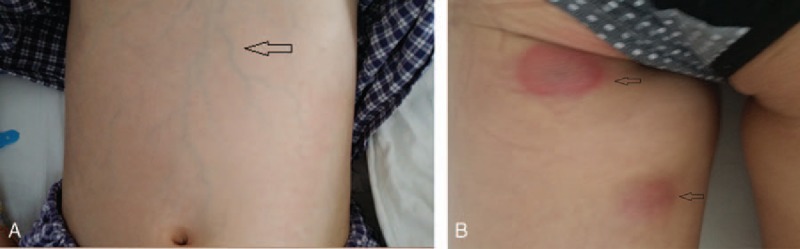
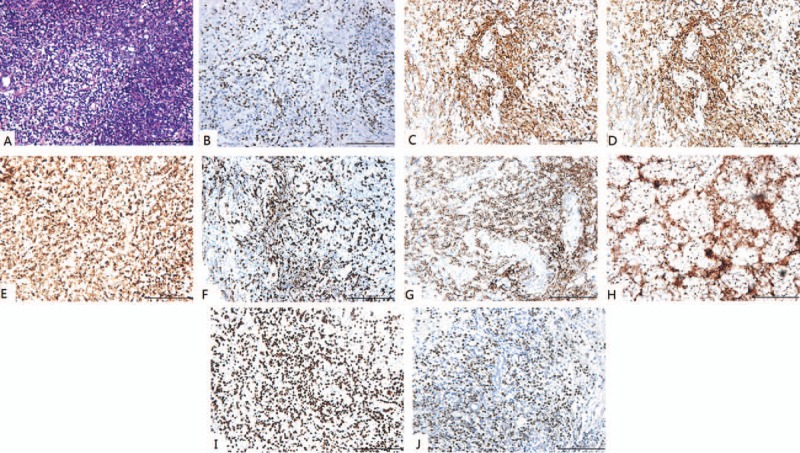
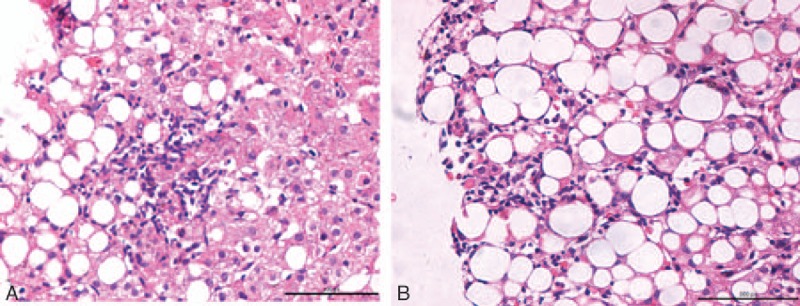
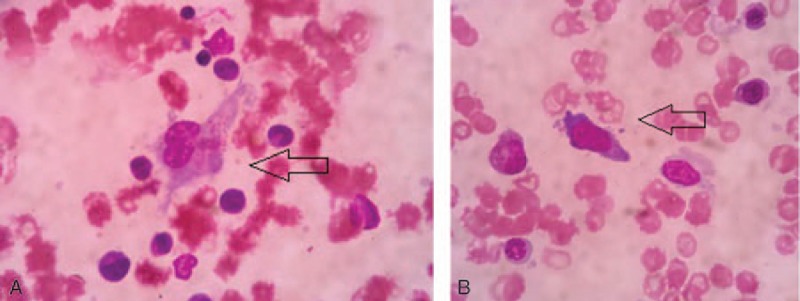
Patient concerns: An 18-year-old girl was admitted to our hospital with a history of edema in the lower limbs and intermittent fever lasting for more than 1 month. At admission, she had severe liver injury of unknown etiology. Laboratory test results revealed pancytopenia, hyperferritinemia, hypertriglyceridemia, and hypofibrinogenemia. Results of serologic tests for EBV were positive. Results of a skin biopsy indicated EBV-positive NK/T-cell lymphoma, and bone marrow aspiration revealed focal hemophagocytosis and atypical lymphoid cells.
Diagnosis: On the basis of these findings, we diagnosed the case as extra-nodal NK/T-cell lymphoma-associated HPS (natural killer/T-cell lymphoma-associated hemophagocytic syndrome), which is commonly induced by CAEBV.
Interventions: Treatment consisted of general management of hepatitis, supplemented with albumin and empirical antibiotic therapy.
Outcomes: The patient died from massive gastrointestinal hemorrhage a week after she was discharged from the hospital.
Lessons: ENKL and HPS present with varied features and are generally fatal; therefore, clinicians should proceed with caution in suspected cases. HPS should be considered when the patient presents with fever, hepatosplenomegaly, pancytopenia, and liver failure. When HPS is suspected, clinicians should determine the underlying cause, such as severe infection, including infection with viruses such as EBV; genetic predisposition; or underlying malignancies, especially lymphoma because of its strong association with HPS.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Zhang T, Fu Q, Gao D, et al. EBV associated lymphomas in 2008 WHO classification. Pathol Res Pract 2014;210:69–73. - PubMed
-
- Williams H, Crawford DH. Epstein–Barr virus: the impact of scientific advances on clinical practice. Blood 2006;107:862–9. - PubMed
-
- Ohshima K, Kimura H, Yoshino T, et al. Proposed categorization of pathological states of EBV-associated T/natural killer-cell lymphoproliferative disorder (LPD) in children and young adults: overlap with chronic active EBV infection and infantile fulminant EBV T-LPD. Pathol Int 2008;58:209–17. - PubMed
-
- Park S, Ko YH. Epstein–Barr virus-associated T/natural kill-cell lymphoproliferative disorders. J Dermatol 2014;41:29–39. - PubMed
-
- Leeborg N, Russell T, Fan G. Systemic Epstein–Barr virus-positive T-cell lymphoproliferative disease of childhood. Pathol Case Rev 2012;17:120–4.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
